Inhoud herevaluatie behandeling BPPD
Uitgangsvraag
Hoe zou de evaluatie van de BPPD behandeling eruit moeten zien?
Aanbeveling
Bij falen van de behandeling moet geëvalueerd worden of de patiënt 1) persisterende of andersoortige BPPD heeft 2) co-existente vestibulaire aandoeningen heeft die geïdentificeerd en behandeld moeten worden en 3) een centrale aandoening heeft.
Overwegingen
- Voordeel: het opstellen van een effectief behandelplan voor patiënten met persisterende BPPD en comorbiditeiten, afname in de kans op het missen van ernstige aandoeningen die een andere behandeling vereisen.
- Nadeel: geen
- Kosten: kosten van herevaluatie en vervolgtesten
- Afweging: de voordelen wegen op tegen de nadelen.
- Waarde oordeel: behandeling van BPPD en andere vestibulaire aandoeningen die in combinatie kunnen voorkomen; behandeling van persisterende BPPD met een repositie manoeuvre na expectatief beleid of vestibulaire revalidatie.
- Rol van de voorkeur van de patiënt: minimaal
Onderbouwing
|
Niveau 4 |
Bij falen van de behandeling kan er sprake zijn van 1) persisterende of andersoortige BPPD 2) co-existente vestibulaire aandoening 3) centrale aandoening.
|
Although the repositioning maneuvers have a substantial success rate, they are not expected to solve the at yet unknown origin of clod or debris formation, which may explain the substantial number of re/occurrences of BPPV. Patients with persistent symptoms of vertigo, dizziness, or unsteadiness at the time of reassessment of the initial treatment response are classified as treatment failures. Treatment failures require reevaluation for the following reasons: 1) Persistent BPPV may be present and responsive to additional maneuvers; 2) coexisting vestibular conditions may be present that can be identified and treated; and 3) serious CNS disorders may simulate BPPV and need to be identified (Furman, et al., 1995) (Furman, et al., 1999) (Rupa, et al., 2004).
Persistent BPPV
Patients with BPPV who initially are treated with observation may fail to resolve spontaneously and have persistent BPPV at the time reassessment. Also, on the basis of failure rates of vestibular rehabilitation or a single-session PRM ranging from 15 to 50 percent, a significant number of patients initially managed with vestibular rehabilitation or PRM will have persistent BPPV at reassessment, which also indicates a treatment failure Furman, et al., 1999) (Hilton, et al., 2004) (Cohen, et al., 2005) (Teixeira, et al., 2006) (von Brevern, et al., 2006). Reevaluation of a treatment failure should include obtaining a history of vertigo, determining if the vertigo is provoked by positional change relative to gravity (ie, lying down in bed, rolling over, bending down, or tilting the head back), which then suggests persistent BPPV. As with the original diagnostic criteria, the Dix-Hallpike test should be repeated to confirm the diagnosis of BPPV. If the Dix-Hallpike maneuver is still positive, repeat PRMs can then be performed as a preferred treatment. The rate of successful treatment of BPPV reaches 90 to 98 percent when additional repositioning maneuvers are subsequently performed (Brocchetti, et al., 2003) (Beynon, et al., 2000). Therefore, the PRMs are the treatment of choice for initial BPPV treatment failures deemed to be due to persistent BPPV.
A similar approach may be adopted for the reevaluation of persistent symptoms of vertigo after an initial diagnosis of lateral canal BPPV. The supine roll test should be repeated and, if characteristic nystagmus is elicited, a PRM appropriate for lateral canal BPPV may be repeated as well. There are limited data regarding the management of treatment failures after PRM for lateral canal BPPV, because this condition seems to respond more consistently to PRM and it also has a higher spontaneous resolution rate (Tirelli, et al., 2004) (Sekine, et al., 2006) (Fife, et al., 1998) (Asprella Libonati, et al., 2005). Some studies indicate cure rates of 86 to 100 percent with up to four PRM treatments in lateral canal BPPV (Casani, et al., 2002) (Chiou, et al., 2005). Further subanalysis suggests that the apogeoptropic variant of lateral canal BPPV may be more refractory to therapy (White, et al., 2005) (Casani, et al., 2002).
A small percentage of patients initially diagnosed and treated for lateral canal BPPV or horizontal canal BPPV may experience a canal switch. In these cases, initial horizontal canal BPPV may transform into posterior canalBPPV in up to 6 percent of cases (Nuti, et al., 1998) (Tirelli, et al., 2004). Similarly, a small fraction of patients (also approximating 6%) initially presenting with posterior canal BPPV may transition after treatment to lateral canal BPPV (Yimtae, et al., 2003) (Herdman, et al., 1996). A small subset of patients who do not respond to treatment for posterior canal and/or lateral canal BPPV may suffer from anterior canal BPPV, and may need to be evaluated accordingly (Jackson, et al., 2007). Finally, although rare, two semicircular canals may be simultaneously involved. The second canal’s involvement may become evident at the time of reassessment if one of the involved canals was appropriately treated (Rupa, et al., 2004). Thus, reassessment of persistent positional vertigo in BPPV should include examination for involvement of other semicircular canals than originally diagnosed. Coexisting Vestibular System Dysfunction A BPPV treatment failure subsequently may be found to be a case manifesting vertiginous symptoms that are provoked by head and body movements in general (ie, not primarily provoked by positional changes relative to gravity); unprovoked (ie, spontaneous) episodes of vertigo occurring while not moving; or in fact, a constant unsteadiness. These specific findings should be identified by clinicians at the time of reevaluation; such findings suggest the presence of vestibular system dysfunction associated with or in addition to the initially treated BPPV. There may be several possible factors at play when vestibular system dysfunction accompanies BPPV.
In a study by Monobe et al, (Monobe, et al., 2001) treatment failure of the PRM was most commonly seen in patients with BPPV secondary to head trauma or vestibular neuritis. Because vestibular neuritis and head trauma are both frequently associated with vestibular dysfunction, the cause of persistent symptoms following treatment of BPPV is likely related to widespread dysfunction within the vestibular system in this setting (Bergenius, et al., 1999). Because BPPV is more common in patients with Ménière’s disease and migraine, vestibular system dysfunction associated with these disorders can lead to prolonged symptoms of BPPV, greater chance for recurrence of BPPV, and increased risk for falls, particularly in older persons (Gordon, et al., 2004) (Roberts, et al., 2005) (Hughes, et al., 1997) (Dornhoffer, et al., 2000) (Uneri, et al., 2004) (Kayan, et al., 1984).
In addition, BPPV not associated with any other ontological or neurological disease can still be associated with an underlying impaired vestibular function, and these individuals are more likely to have incomplete resolution of symptoms even if their Dix-Hallpike testing normalizes with PRM (Pollak, et al., 2002). Finally, transient vestibular dysfunction can also occur following repositioning maneuvers. Evidence suggests that balance function continues to be affected between 1 to 3 months after repositioning maneuvers, and that some of these patients may need additional balance therapy (ie, counseling, vestibular rehabilitation) to prevent falls and decrease their fear of falling after the vertigo from BPPV has resolved (Blatt, et al., 2000) (Chang, et al., 2006) (Giacomini, et al., 2002) (Black, et al., 1984). Thus, reevaluation of BPPV treatment failures should include a search for these associated conditions.
When coexisting vestibular system dysfunction is suspected, additional testing should be considered. This testing may include audiometric testing to screen for Ménière’s disease and nerve VIII pathology such as acoustic neuroma, vestibular function testing to detect central and peripheral vestibular dysfunction, and CNS imaging to detect CNS pathology. Such subsequent testing will need to be tailored to the clinical presentation, and clinicians should exercise their clinical judgment. Vestibular rehabilitation has been shown to be an effective treatment for vestibular symptoms due to the potentially persistent vestibular dysfunction associated with BPPV; this treatment may reduce the risk for falls (Angeli, et al., 2003).
CNS Disorders Masquerading as BPPV Although vertigo of central origin is frequently associated with neurological symptoms such as gait, speech, and autonomic dysfunction, it is important to recognize that, rarely, CNS disorders can masquerade as BPPV (Bertholon, et al., 2002). Many of these have been previously discussed in the section on differential diagnosis, but the relative likelihood of their diagnosis increases in the face of initial treatment failure. In one study, a CNS disorder that explained BPPV treatment failure was found in 3 percent of patients (Dal, et al., 2000).
Whenever the signs and symptoms of BPPV are atypical or refractory to treatment, additional history and physical examination should be obtained to address the possibility of undiagnosed CNS disease (Smouha, et al., 1995). Patients with symptoms consistent with those of BPPV who do not show improvement or resolution after undergoing the PRM, especially after two or three attempted maneuvers, or those who describe associated auditory or neurological symptoms should be evaluated with a thorough neurological examination, additional CNS testing, and/or MRI of the brain and posterior fossa to identify possible intracranial pathological conditions (Dunniway, et al., 1998) (Buttner, et al., 1999).
- Angeli, S.I., Hawley, R., Gomez, O. (2003). Systematic approach to benign paroxysmal positional vertigo in the elderly. Otolaryngol Head Neck Surg, 128, 719-25.
- Asprella Libonati, G. (2005). Diagnostic and treatment strategy of lateral semicircular canal canalolithiasis. Acta Otorhinolaryngol Ital, 25, 277-83.
- Bergenius, J., Perols, O. (1999). Vestibular neuritis: a follow-up study. Acta Otolaryngol, 119, 895-9.
- Bertholon, P., Bronstein, A.M., Davies, R.A., et al. (2002). Positional down beating nystagmus in 50 patients: cerebellar disorders and possible anterior semicircular canalithiasis. J Neurol Neurosurg Psychiatry, 72, 366-72.
- Beynon, G.J., Baguley, D.M., da Cruz, M.J. (2000). Recurrence of symptoms following treatment of posterior semicircular canal benign positional paroxysmal vertigo with a particle repositioning manoeuvre. J Otolaryngol, 29, 2-6.
- Black, F.O., Nashner, L.M. (1984). Postural disturbance in patients with benign paroxysmal positional nystagmus. Ann Otol Rhinol Laryngol, 93, 595-9.
- Blatt, P.J., Georgakakis, G.A., Herdman, S.J., et al. (2000). The effect of the canalith repositioning maneuver on resolving postural instability in patients with benign paroxysmal positional vertigo. Am J Otol, 21, 356-63.
- von Brevern, M., Seelig, T., Radtke, A., et al. (2006). Short-term efficacy of Epley’s manoeuvre: a double-blind randomised trial. J Neurol Neurosurg Psychiatry, 77, 980-2.
- Brocchetti, F., Garaventa, G., Ameli, F., et al. (2003). Effect of repetition of Semont’s manoeuvre on benign paroxysmal positional vertigo of posterior semicircular canal. Acta Otorhinolaryngol Ital, 23, 428-35.
- Buttner, U., Helmchen, C., Brandt, T. (1999). Diagnostic criteria for central versus peripheral positioning nystagmus and vertigo: a review. Acta Otolaryngol, 119, 1-5.
- Casani, A.P., Vannucci, G., Fattori, B., et al. (2002). The treatment of horizontal canal positional vertigo: our experience in 66 cases. Laryngoscope, 112, 172-8.
- Chang, W.C., Hsu, L.C., Yang, Y.R., et al. (2006). Balance ability in patients with benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg, 135, 534-40.
- Chiou, W.Y., Lee, H.L., Tsai, S.C., et al. (2005). A single therapy for all subtypes of horizontal canal positional vertigo. Laryngoscope, 115, 1432-5.
- Cohen, H.S., Kimball, K.T. (2005). Effectiveness of treatments for benign paroxysmal positional vertigo of the posterior canal. Otol Neurotol, 26, 1034-40.
- Dal, T., Ozluoglu, L.N., Ergin, N.T. (2000). The canalith repositioning maneuver in patients with benign positional vertigo. Eur Arch Otorhinolaryngol, 257, 133-6.
- Dornhoffer, J.L., Colvin, G.B. (2000). Benign paroxysmal positional vertigo and canalith repositioning: clinical correlations. Am J Otol, 21, 230-3.
- Dunniway, H.M., Welling, D.B. (1998). Intracranial tumors mimicking benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg, 118, 429-36.
- Fife, T.D. (1998). Recognition and management of horizontal canal benign positional vertigo. Am J Otol, 19, 345-51.
- Froehling, D.A., Bowen, J.M., Mohr, D.N., et al. (2000). The canalith repositioning procedure for the treatment of benign paroxysmal positional vertigo: a randomized controlled trial. Mayo Clin Proc, 75, 695-700.
- Furman, J.M., Cass, S.P. (1999). Benign paroxysmal positional vertigo. N Engl J Med, 341, 1590-6.
- Furman, J.M., Cass, S.P. (1995). A practical work-up for vertigo. Contemp Intern Med, 7, 24-7.
- Giacomini, P.G., Alessandrini, M., Magrini, A. (2002). Long-term postural abnormalities in benign paroxysmal positional vertigo. ORL J Otorhinolaryngol Relat Spec, 64, 237-41.
- Gordon, C.R., Levite, R., Joffe, V., et al. (2004). Is posttraumatic benign paroxysmal positional vertigo different from the idiopathic form?. Arch Neurol, 61, 1590-3.
- Helminski, J.O., Janssen, I., Kotaspouikis, D., et al. (2005). Strategies to prevent recurrence of benign paroxysmal positional vertigo. Arch Otolaryngol Head Neck Surg, 131, 344-8.
- Herdman, S.J., Tusa, R.J. (1996). Complications of the canalith repositioning procedure. Arch Otolaryngol Head Neck Surg, 122, 281-6.
- Hilton, M., Pinder, D. (2004). The Epley (canalith repositioning) manoeuvre for benign paroxysmal positional vertigo. Cochrane Database Syst Rev, 0, CD003162-.
- Hughes, C.A., Proctor, L. (1997). Benign paroxysmal positional vertigo. Laryngoscope, 107, 607-13.
- Jackson, L.E., Morgan, B., Fletcher, J.C., Jr., et al. (2007). Anterior canal benign paroxysmal positional vertigo: an underappreciated entity. Otol Neurotol, 28, 218-22.
- Kayan, A., Hood, J.D. (1984). Neuro-otological manifestations of migraine. Brain, 107, 1123-42.
- Lynn, S, Lynn, S., Pool, A., Rose, D., et al. (0000). Randomized trial of the canalith repositioning procedure. Otolaryngol Head Neck Surg, 113, 712-720.
- Magliulo, G., Bertin, S., Ruggieri, M., et al. (2005). Benign paroxysmal positional vertigo and post-treatment quality of life. Eur Arch Otorhinolaryngol, 262, 627-30.
- Monobe, H., Sugasawa, K., Murofushi, T. (2001). The outcome of the canalith repositioning procedure for benign paroxysmal positional vertigo: are there any characteristic features of treatment failure cases?. Acta Otolaryngol Suppl, 545, 38-40.
- Munoz, J.E., Miklea, J.T., Howard, M., et al. (2007). Canalith repositioning maneuver for benign paroxysmal positional vertigo: randomized controlled trial in family practice. Can Fam Physician, 53, 1049-53.
- Nunez, R.A., Cass, S.P., Furman, J.M. (2000). Short- and long-term outcomes of canalith repositioning for benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg, 122, 647-52.
- Nuti, D., Agus, G., Barbieri, M.T., et al. (1998). The management of horizontalcanal paroxysmal positional vertigo. Acta Otolaryngol, 118, 455-60.
- Pollak, L., Davies, R.A., Luxon, L.L. (2002). Effectiveness of the particle repositioning maneuver in benign paroxysmal positional vertigo with and without additional vestibular pathology. Otol Neurotol, 23, 79-83.
- Roberts, R.A., Gans, R.E., Kastner, A.H., et al. (2005). Prevalence of vestibulopathy in benign paroxysmal positional vertigo patients with and without prior otologic history. Int J Audiol, 44, 191-6.
- Rupa, V. (2004). Persistent vertigo following particle repositioning maneuvers: an analysis of causes. Arch Otolaryngol Head Neck Surg, 130, 436-9.
- Sekine, K., Imai, T., Sato, G., et al. (2006). Natural history of benign paroxysmal positional vertigo and efficacy of Epley and Lempert maneuvers. Otolaryngol Head Neck Surg, 135, 529-33.
- Sherman, D., Massoud, E.A. (2001). Treatment outcomes of benign paroxysmal positional vertigo. Journal of Otolaryngology, 30, 295-9.
- Smouha, E.E., Roussos, C. (1995). Atypical forms of paroxysmal positional nystagmus. Ear Nose Throat J, 74, 649-56.
- Teixeira, L.J., Machado, J.N. (2006). Maneuvers for the treatment of benign positional paroxysmal vertigo: a systematic review. Rev Bras Otorrinolaringol (Engl Ed), 72, 130-9.
- Tirelli, G., Russolo, M. (2004). 360-Degree canalith repositioning procedure for the horizontal canal. Otolaryngol Head Neck Surg, 131, 740-6.
- Uneri, A. (2004). Migraine and benign paroxysmal positional vertigo: an outcome study of 476 patients. Ear Nose Throat J, 83, 814-5.
- White, J.A., Coale, K.D., Catalano, P.J., et al. (2005). Diagnosis and management of lateral semicircular canal benign paroxysmal positional vertigo. Otolaryngol Head Neck Surg, 133, 278-84.
- Woodworth, B.A., Gillespie, M.B., Lambert, P.R. (2004). The canalith repositioning procedure for benign positional vertigo: a meta-analysis. Laryngoscope, 114, 1143-6.
- Yimtae, K., Srirompotong, S., Sae-Seaw, P. (2003). A randomized trial of the canalith repositioning procedure. Laryngoscope, 113, 828-32.
Beoordelingsdatum en geldigheid
Publicatiedatum : 20-08-2013
Beoordeeld op geldigheid : 01-02-2020
De tekst van deze module is opgesteld tijdens de richtlijnontwikkeling in 2010 door de oorspronkelijke richtlijnwerkgroep (zie Samenstelling werkgroep). De module is opnieuw beoordeeld en nog actueel bevonden door de werkgroep samengesteld voor de richtlijnherziening in 2019 (zie samenstelling huidige werkgroep). Uiterlijk in 2024 bepaalt het bestuur van de Nederlandse Vereniging voor Keel-Neus-Oorheelkunde en Heelkunde van het Hoofd-Halsgebied of de richtlijnmodule nog actueel is.
Algemene gegevens
Met ondersteuning van de Orde van Medisch Specialisten. De richtlijnontwikkeling werd gefinancierd uit de Stichting Kwaliteitsgelden Medisch Specialisten (SKMS).
De richtlijn betreft een adaptatie van:
Clinical practice guideline: Benigne Paroxysmale Positionele Duizeligheid.
De Amerikaanse richtlijn van de Academy of Otolaryngology-Head and Neck surgery foundation ‘Clinical practice guideline: Benign paroxysmal positional vertigo’ (Bhattacharayya, et al., 2008) vormde het uitgangspunt van de onderhavige richtlijn. Daarnaast werd de Amerikaanse richtlijn van de Academy of neurology, gericht op de behandeling van BPPD, gebruikt ter aanvulling (Fife, et al., 2008), alsmede de discussies en richtlijnen van de Standaardisatie commissie van de Barany Society (Reykjavik, et al., 2010, www.baranysociety.nl).
Doel en doelgroep
De primaire doelstellingen van deze richtlijn zijn:
- De kwaliteit van de zorg te verbeteren door middel van een accurate en snelle diagnose van BPPD.
- Voorkomen van onnodig gebruik van medicijnen.
- Doelgericht gebruik van aanvullend onderzoek.
- Stimuleren van het gebruik van repositiemanoeuvres als therapie voor BPPD.
Secundaire doelstellingen zijn: beperking van de kosten van diagnose en behandeling van BPPD, vermindering van het aantal artsenbezoeken, en verbetering van de kwaliteit van leven. Het grote aantal patiënten met BPPD en de verscheidenheid aan diagnostische en therapeutische interventies voor BPPD maakt dit een geschikt onderwerp voor een evidence-based richtlijn.
De Amerikaanse richtlijn van de Academy of Otolaryngology-Head and Neck surgery foundation ‘Clinical practice guideline: Benign paroxysmal positional vertigo’ (Bhattacharayya, et al., 2008) vormde het uitgangspunt van de onderhavige richtlijn. Daarnaast werd de Amerikaanse richtlijn van de Academy of neurology, gericht op de behandeling van BPPD, gebruikt ter aanvulling (Fife, et al., 2008), alsmede de discussies en richtlijnen van de Standaardisatie commissie van de Barany Society (Reykjavik, et al., 2010, www.baranysociety.nl)). Onze doelstelling was om deze multidisciplinaire richtlijn te adapteren aan de Nederlandse situatie met behulp van Nederlandse input, waarbij de aanbevelingen rekening houden met wetenschappelijk bewijs en zich richten op harm-benefit balans, en expert consensus om de gaten in wetenschappelijk bewijs op te vullen. Deze specifieke aanbevelingen kunnen dan gebruikt worden om indicatoren te ontwikkelen en te gebruiken voor kwaliteitsverbetering.
Deze richtlijn is opgesteld voor KNO-artsen en neurologen die in hun klinische praktijk in aanraking komen met BPPD. De richtlijn is toepasbaar in iedere setting waar BPPD gediagnosticeerd en behandeld wordt.
Samenstelling werkgroep
Voor het ontwikkelen van de module is in 2018 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen die betrokken zijn bij de zorg voor patiënten met BPPD.
De werkgroepleden zijn door hun beroepsverenigingen gemandateerd voor deelname. De werkgroep is verantwoordelijk voor de integrale tekst van deze module.
Samenstelling huidige werkgroep:
- Dr. Tj.D. (Tjasse) Bruintjes, KNO-arts, Gelre Ziekenhuizen, Apeldoorn, NVKNO (voorzitter)
- Dr. R.B. (Roeland) van Leeuwen, neuroloog, Gelre ziekenhuizen, Apeldoorn, NVN
- Dr. R. (Raymond) van de Berg, KNO-arts/vestibuloloog, Maastricht UMC+, Maastricht, NVKNO
- Dr. M. (Marloes) Thoomes-de Graaf, fysiotherapeut/manueel therapeut/klinisch epidemioloog, Fysio-Experts, Hazerswoude, KNGF en NVMT
- R.A.K. (Sandra) Rutgers, arts, MPH en voorzitter Commissie Ménière Stichting Hoormij, Houten, Stichting Hoormij
Met ondersteuning van:
- D. (Dieuwke) Leereveld, MSc., senior adviseur Kennisinstituut van de Federatie Medisch Specialisten
- Drs. M. (Monique) Wessels, informatiespecialist Kennisinstituut van de Federatie Medisch Specialisten
Samenstelling oorspronkelijke werkgroep (2010):
- dr. Tj.D. Bruintjes (voorzitter), KNO-arts, Gelre ziekenhuizen, Apeldoorn
- prof. dr. H. Kingma, klinisch fysicus/vestibuloloog, Maastricht Universitair Medisch Centrum en Technische Universiteit Eindhoven
- dr. D.J.M. Mateijsen, KNO-arts, Catharina ziekenhuis, Eindhoven
- dr. R.B. van Leeuwen, neuroloog, Gelre ziekenhuizen, Apeldoorn
- dr. ir. T van Barneveld klinisch epidemioloog, Orde van Medisch specialisten (adviseur)
- dr. M.L. Molag, Orde van Medisch specialisten (adviseur)
Belangenverklaringen
De werkgroepleden hebben onafhankelijk gehandeld en waren vrij van financiële of zakelijke belangen betreffende het onderwerp van de richtlijn.
Methode ontwikkeling
Evidence based
Werkwijze
De Amerikaanse richtlijn van de Academy of Otolaryngology-Head and Neck surgery foundation ‘Clinical practice guideline: Benign paroxysmal positional vertigo’ (Bhattacharayya, et al., 2008) vormde het uitgangspunt van de onderhavige richtlijn. Daarnaast werd de Amerikaanse richtlijn van de Academy of neurology gebruikt (Fife, et al., 2008). Dit betekent dat de Nederlandse richtlijncommissie de studies, de beoordeling & gradering ervan en de begeleidende tekst heeft overgenomen. Studies, relevant voor dit onderwerp, die nadien werden gepubliceerd konden in de richtlijncommissie worden ingebracht. De literatuur werd bovendien geupdate door te zoeken in Medline naar nieuw verschenen systematische reviews en RCTs met als onderwerp BPPD in de periode van 2008 t/m 2010.
De richtlijncommissie is voor elke aanbeveling in de Amerikaanse richtlijn nagegaan welke overwegingen naast het wetenschappelijk bewijs zijn gebruikt en of de door de commissie aangedragen studies de aanbeveling zouden kunnen veranderen. Wanneer er consensus was over deze overwegingen en door de commissie aangedragen studies geen ander inzicht opleverden, zijn de aanbevelingen overgenomen. Indien de commissie andere overwegingen (ook) van belang achtte of meende dat de door haar aangedragen studies een (iets) ander licht wierpen op de in de Amerikaanse richtlijn vermelde aanbeveling, zijn de aanbevelingen gemodificeerd.
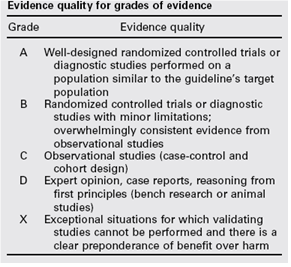
De gradering van de studies in de Amerikaanse richtlijn wijkt af van wat hier te lande gangbaar is. Vanuit het oogpunt van uniformiteit achtte de Nederlandse commissie het wenselijk de classificatie van bewijs c.q. gradering te converteren naar de Nederlandse classificatie. De Amerikaanse classificatie is hieronder afgebeeld in tabel. De corresponderende “Nederlandse” classificatie is in tabel 1.2 opgenomen.
Tabel 1.1: gradering van de studies in de Amerikaanse richtlijn
Tabel 1.2 Relatie tussen Evidence quality for grades of evidence en niveau van conclusie op basis van kwaliteit van bewijs conform Classificatieschema van CBO.
|
Evidence Quality - symbool |
Evidence Quality – omschrijving |
Niveau van conclusie – symbool |
Niveau van conclusie omschrijving |
|
A
|
Well-designed randomized controlled trials or diagnostic studies performed on a population similar to the guideline’s target population |
1 |
Meerdere gerandomiseerde dubbelblinde vergelijkende klinisch onderzoeken van goede kwaliteit van voldoende omvang, of
Meerdere onderzoeken ten opzichte van een referentietest (een ‘gouden standaard’) met tevoren gedefinieerde afkapwaarden en onafhankelijke beoordeling van de resultaten van test en gouden standaard, betreffende een voldoende grote serie van opeenvolgende patiënten die allen de index- en referentietest hebben gehad |
|
B |
Randomized controlled trials or diagnostic studies with minor limitations; overwhelmingly consistent evidence from observational studies |
2 |
Meerdere vergelijkende onderzoeken, maar niet met alle kenmerken als genoemd onder 1 (hieronder valt ook patiënt-controle onderzoek, cohort-onderzoek), of
Meerdere onderzoeken ten opzichte van een referentietest, maar niet met alle kenmerken die onder 1 zijn genoemd. |
|
C |
Observational studies (case-control and cohort design) |
||
|
D |
Expert opinion, case reports, reasoning from first principles (bench research or animal studies) |
3 en 4 |
Niet vergelijkend onderzoek of mening van deskundigen |
In de Amerikaanse richtlijn worden ook de aanbevelingen gegradeerd in termen van ‘strong recommendation’, ‘recommendation’, ‘option’. Hier te lande is graderen van aanbevelingen niet gebruikelijk. Om deze reden zijn in de Nederlandse richtlijn de aanbevelingen niet gegradeerd.
De literatuurzoekstrategie die de Amerikaanse richtlijncommissie heeft gevolgd, staat in bijlage 1 beschreven. Voor het opstellen van de aanbevelingen heeft de Amerikaanse richtlijncommissie gebruik gemaakt van de GuideLine Implementability Appraisal (GLIA) tool. Dit instrument dient om de helderheid van de aanbevelingen te verbeteren en potentiële belemmeringen voor de implementatie te voorspellen. In bijlage 3 wordt een aantal criteria beschreven. Ook de Nederlandse richtlijncommissie heeft deze criteria gehanteerd.