Laparoscopie
Uitgangsvraag
Wat is de rol van laparoscopie bij de behandeling van abdominaal letsel na trauma?
Aanbeveling
Voer bij hemodynamisch instabiele traumapatiënten met abdominaal letsel een traumalaparotomie uit.
Overweeg laparoscopie bij geselecteerde hemodynamisch stabiele patiënten met discrepantie tussen klinisch beeld en beeldvorming. Hierbij dient rekening gehouden te worden met de aard van het letsel en de aanwezige expertise ten aanzien van het adequaat en veilig uitvoeren van een laparoscopie.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
Van oudsher is de traumalaparotomie de gouden standaard bij abdominaal trauma waarbij er een indicatie bestaat voor operatief ingrijpen. De laatste jaren komt er steeds meer aandacht voor de rol van laparoscopie. De systematische review van Cirocchi (2018) concludeert op basis van de geïncludeerde studies, die zijn uitgevoerd in verschillende traumacentra wereldwijd, dat het aantal laparoscopieën in traumapatiënten (vanaf 1990) is toegenomen en het aantal laparotomieën is afgenomen. Er is daarom literatuuronderzoek gedaan naar de rol van laparoscopie bij de behandeling van abdominaal trauma. Hoewel er veel literatuur beschikbaar is, is het meeste van retrospectief karakter met een beperkte kwaliteit, waarbij onduidelijkheid is over de aanwezige letsels en/of de ernst van het letsel in beide groepen vergelijkbaar waren. Hierdoor kunnen er geen sterke conclusies getrokken worden over het effect van laparoscopie op de gedefinieerde uitkomstmaten (gemist letsel, mortaliteit, re-interventies, complicaties, kwaliteit van leven). Ondanks de (zeer) lage bewijskracht, laat de geïncludeerde literatuur wel een aantal trends zien; in geval van een hemodynamisch stabiele patiënt lijkt een laparoscopie niet gepaard te gaan met een verhoogde kans op gemist letsel. Daarnaast suggereren de meeste studies dat in zowel de patiënten behandeld met laparoscopie, als de patiënten behandeld met traumalaparotomie het risico op mortaliteit en complicaties laag is. Al is er ook een klein deel van de studies dat een hoger mortaliteitsrisico suggereert bij traumalaparotomie. Dit kan mogelijk worden verklaard omdat de ernstigere traumapatiënten eerder een traumalaparotomie ondergaan.
Er is bij laparoscopie wel een kans op conversie naar laparotomie (tot 45% beschreven). Dit is afhankelijk van het aanwezige intra-abdominale letsel en ervaring van de chirurg. Echter zijn de consequenties van een niet-therapeutische of negatieve laparotomie groter in vergelijking met een niet-therapeutische of negatieve laparoscopie. Er is bij de laparoscopie sprake van minder complicaties (wondinfectie, pneumonie, adhesies en littekenbreuken) en verkorte opname duur (Sermonesie, 2023; Smyth 2022). Laparoscopie gaat wel gepaard met mogelijk langere OK duur, lastigere procedures waarbij ervaring van belang is en mogelijk toegenomen gemist letsel in geval van weinig laparoscopische ervaring. Echter, de nauwkeurigheid van de laparoscopie neemt in de afgelopen jaren toe. De beschreven studies laten zien dat het aantal gemiste letsels door laparoscopie in de recente studies vergelijkbaar is met de laparotomie en bedraagt circa 0,5% (Alzarouni, 2022; Gomez, 2022; Wang, 2022). Daarnaast wordt laparoscopie als behandel modaliteit steeds meer gebruikt en geaccepteerd door de toename in vaardigheden, hecht en stapler technieken en het gebruik van devices; met name gericht op intracorporeel hechten/anastomoseren van darmen.
In het overgrote deel van de geïncludeerde studies bestond de studiepopulatie uit hemodynamisch stabiele patiënten en conclusies kunnen dus alleen worden getrokken over deze patiëntengroep. Dit is lijn met resultaten met andere studies, waaronder het review van Ki (2021; 19 studies geïncludeerd, n = 1520) waarin wordt geconcludeerd dat laparoscopie een veilige optie is in hemodynamisch stabiele patiënten met stomp abdominaal trauma. Ook de laatste WSES-guideline (Smyth, 2022) naar darmletsel ten gevolge van trauma geeft aan dat er wel degelijk plaats is voor laparoscopie in de behandeling van traumatisch darmletsel (WSES-guideline: GRADE Moderate). Ook het laatste WSES-consensus statement (Sermonesi, 2023) luidt dat laparoscopie overwogen mag worden als eerste behandelkeuze in geval van abdominaal trauma (WSES-consensus statement: Moderate quality evidence, 1B). Het review door Wang (2022) heeft een subgroep analyse verricht tussen de patiënten met penetrerend vs. stomp abdominaal trauma, hierbij wordt geen verschil gevonden als het gaat om mortaliteit, gemist letsels of complicaties.
Bij hemodynamische instabiliteit ondergaat de patiënt een traumalaparotomie omdat met een laparotomie het snelst en het best een totaaloverzicht en controle verkregen kan worden over de abdominale letsels. In bijna geen enkele geïncludeerde studie werd laparoscopie uitgevoerd in de hemodynamisch instabiele patiënten.
We zien door de toegenomen nauwkeurigheid van de CT-scan een afname in de indicatie voor een diagnostische laparoscopie. Wel wordt het doorgaans een diagnostische laparoscopie verricht indien er een discrepantie bestaat tussen de negatieve bevindingen op de CT en de klinische presentatie of de aard van het ongevalsmechanisme. Bij geen eenduidig beeld op CT of geen overeenstemming met de aard van het trauma en kliniek kan een diagnostische laparoscopie worden verricht. De uitkomst van een laparoscopische ingreep wordt in belangrijke mate bepaald door de operatieve vaardigheden van de operateur. Dit verklaart dan ook mede de variatie in uitkomsten van studies die laparoscopie versus open in de behandeling van abdominale letsels bij de hemodynamisch stabiele patiënt. Hoewel in de meest recente studies zeer lage complicatie percentages worden beschreven moeten we ons realiseren dat deze studies zijn uitgevoerd door chirurgen die waarschijnlijk uitgebreide ervaring in laparoscopisch opereren hebben.
Waarden en voorkeuren van patiënten (en evt. hun verzorgers)
Een groot voordeel van laparoscopie, is dat complicaties van een traumalaparotomie mogelijk voorkomen worden en gepaard gaat met een kortere opname duur. In een deel van de patiënten is conversie van laparoscopie naar laparotomie nodig, de literatuur laat percentages zien die variëren tot 45%. Bij de overige patiënten is mogelijk een laparotomie bespaard gebleven. Ondanks de eventuele voordelen van een laparoscopie, dient per individuele patiënt afgewogen te worden of uitvoeren van een laparoscopie veilig haalbaar is op basis van kliniek en verwacht letsel. De keuze voor de optimale behandelstrategie dient in afstemming met de patiënt en/of familie of wettelijk vertegenwoordiger te worden gemaakt.
Kosten (middelenbeslag)
Kosteneffectiviteit en duurzaamheid voor de ernstig gewonde patiënt met abdominaal trauma zijn lastige begrippen. Er is een gebrek aan kosten-effectiviteitsstudies van voldoende kwaliteit op basis waarvan onderbouwde uitspraken kunnen worden gedaan over de kosten(effectiviteit) van verschillende behandelmethoden. Niet opereren kan mogelijk goedkoper zijn wel opereren, maar deze financiële afweging kan geen rol spelen in de besluitvorming voor de patiënt met abdominaal trauma. Preventie van non-therapeutische laparotomieën, onnodige minimaal invasieve interventie en re-interventie zijn mogelijk kostenbesparend, maar bovenal beter voor de patiënt. Het primaire doel is de uitkomst van de patiënt te optimaliseren door het verlagen van de mortaliteit, het verminderen van complicaties en re-interventies en het verbeteren van kwaliteit van leven. De invloed van behandelkeuzes op de zorgkosten voor de patiënt met abdominaal trauma en de maatschappij worden derhalve niet in deze richtlijn besproken.
Aanvaardbaarheid, haalbaarheid en implementatie
De richtlijncommissie beveelt aan bij patiënten die voor een laparoscopische benadering in aanmerking komen, en indien dit wenselijk en organisatorisch mogelijk is, een (GE-)chirurg met laparoscopische expertise in de behandeling te betrekken. Het behandelteam voert de laparoscopie uit. Indien laparoscopie niet mogelijk is kan de operateur terug vallen op de laparotomie of laagdrempelig te converteren, indien toch gekozen wordt voor een laparoscopie. Immers veiligheid van de behandeling staat boven de mogelijke gezondheidswinst van een laparoscopische behandeling. Er zou mogelijk gezondheidswinst te behalen zijn bij deze populatie patiënten indien de samenwerking tussen traumachirurg en GE-chirurg zou worden versterkt. Daarbij blijft de traumachirurg steeds regiebehandelaar.
Het zou wenselijk zijn dat de bestaande landelijke traumaregistratie gedurende een korte periode zodanig aangevuld wordt, zodat deze voldoende detail bevat om een transparant overzicht te krijgen van de uitkomsten na behandeling. Met als primair doel om hier meer inzicht in te krijgen, gezien het gebrek aan bewijs over de verschillende behandelopties. Dit kan praktijkvariatie doen afnemen en dienen als spiegelinformatie.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Hoewel afkomstig uit lage kwaliteit studies, suggereert de grote hoeveelheid literatuur naar effectiviteit en veiligheid van een laparoscopie positieve resultaten. Met name voor de hemodynamische stabiele patiënt, kan laparoscopie als een veilig alternatief worden gezien in vergelijking met een traumalaparotomie. De resultaten van een laparoscopie hangen echter sterk af van de expertise en kundigheid van de operateur. Kennis ten aanzien van het adequaat uitvoeren van een laparoscopie zijn cruciaal in de behandelkeuze.
Onderbouwing
Selective non-operative management, diagnostische laparoscopie en een traumalaparotomie zijn beschreven als behandelstrategie van abdominaal letsel ten gevolge van een trauma. Op dit moment bestaat er geen consensus over wanneer een indicatie is voor een laparoscopie dan wel laparotomie. Van een traumalaparotomie wordt beschreven dat dit sneller is en een betere exposure geeft met mogelijk minder gemist letsel tot gevolgd, echter kent een (non-therapeutische) laparotomie ook weer complicaties.
|
Very low GRADE |
The evidence is very uncertain about the effect of laparoscopy on missed injuries, mortality, reintervention, and complications when compared with laparotomy in patients with abdominal trauma.
Source: Wang (2022), Alzarouni (2022), Elkbuli (2022), Gomez (2022) |
Quality of life
|
- GRADE |
No evidence was found regarding the effect of laparoscopy on quality of life when compared with laparotomy in patients with abdominal trauma.
Source: - |
Description of studies
Systematic reviews
Wang (2022) performed a systematic review and meta-analysis to assess the value of diagnostic and therapeutic laparoscopy for patients with blunt or penetrating abdominal trauma. The databases PubMed, Embase and The Cochrane Library were searched for comparative studies on the effectiveness and safety of laparoscopy versus laparotomy for the management of abdominal trauma, published until the 30th of June 2021. The search resulted in 1358 studies of which 23 studies were included in the review. Comparative studies comparing laparoscopy with laparotomy for the management of abdominal trauma were selected. Studies in children (<18 years) were excluded). The 23 included studies encompassed one RCT (Leppaniem and Haapiainen, 2003), two prospective observational studies (DeMaria, 2000; Karateke, 2013), and twenty retrospective observational studies, of which four studies were controlled pre- post studydesigns (Cherkasov, 2008; Lee, 2014; Lin, 2010; Omori, 2003) and sixteen studies had a parallel design (Birindelli, 2021; Chakravartty, 2017; Cherry, 2005; Gao, 2020; Huang, 2017; Khubutiya, 2013; Liao, 2014; Lim, 2015; Lin 2018; Marks, 1997; Miles, 2004; Mutter, 1997; Obaid, 2021; Shams and Elaysi, 2021; Trejo-Avila, 2017). Baseline characteristics of the included studies and patients is presented in Table 1. The study populations of the included studies had both blunt and/or penetrating abdominal trauma. In six of the 23 studies, patients with only penetrating trauma were included (total number of patients n = 3309) and in four of the 23 studies, patients with only blunt trauma were included (total numer of patients n = 445). In ten studies patients with both penetrating and blunt injury were included (number patients not specified), or it was not stated if patients had blunt or penetrating injury. In all except two studies, the study population was hemodynamically stable (Cherkasov, 2008; Chestovich, 2015). The patient age varied from 26 to 57 years, with a 76.9% male population. Outcomes that were reported in the review were conversion from laparoscopy to laparotomy, missed injuries, mortality and complications (wound infection, intra-abdominal abscess, pneumonia, thromboembolism, bowel obstruction or ileus). Risk of bias of the individual studies was assessed with the Cochrane Collaboration’s tool (for the RCTs) and the NewCastle Ottawa Scale (for cohort studies).
Table 1: baseline characteristics of the studies included in the review from Wang (2022)
|
Author |
Year |
Study design |
Country |
N (intervention / control) |
Type of injury |
HD stability Intervention |
HD stability control |
|
Birinidelli |
2021 |
Retrospective parallel |
Italy |
i: 16 / c: 22 |
Splenic trauma |
100% |
100% |
|
Chakravartty |
2017 |
Retrospective parallel |
UK |
i: 25 / c: 25 |
Abdominal trauma |
100% |
100% |
|
Cherkasov |
2008 |
Retrospective pre/post |
Russia |
i: 1332 / c: 1363 |
Penetrating |
100% |
8.7% of total patients |
|
Cherry |
2005 |
Retrospective parallel |
USA |
i: 92/ c: 64 |
Penetrating |
100% |
100% |
|
Chestovich |
2015 |
Retrospective parallel |
USA |
i: 94 / c: 96 |
Penetrating |
100% |
97.9% |
|
DeMaria |
2000 |
Prospective |
USA |
i: 31 / c: 23 |
Abdominal stab wounds |
100% |
100% |
|
Gao |
2020 |
Retrospective parallel |
China |
i: 54 / c: 54 |
Penetrating and Blunt |
100% |
100% |
|
Huang |
2017 |
Retrospective parallel |
USA |
i: 11 / c: 41 |
Blunt |
100% |
100% |
|
Karateke |
2013 |
Prospective |
Turkey |
i: 26 / c: 26 |
Penetrating |
100% |
100% |
|
Khubutiya |
2013 |
Retrospective parallel |
Russia |
i: 328 / c: 280 |
Penetrating and Blunt |
100% |
100% |
|
Lee |
2014 |
Retrospective pre/post |
Taiwan |
i: 57 / c: 47 |
Blunt |
100% |
100% |
|
Leppaniemi and Haapiainen |
2003 |
RCT |
Finalnd |
i: 20 / c: 23 |
Stab wounds |
100% |
100% |
|
Liao |
2014 |
Retrospective parallel |
Taiwan |
i: 15 / c:22 |
Penetrating and Blunt |
100% |
100% |
|
Lim |
2015 |
Retrospective parallel |
South Korea |
i: 41 / c: 55 |
Abdominal trauma |
100% |
100% |
|
Lin |
2018 |
Retrospective parallel |
Taiwan |
i: 126 / c: 139 |
Blunt |
100% |
100% |
|
Lin |
2010 |
Retrospective pre/post |
Taiwan |
i: 48 / c: 38 |
Stab wounds |
100% |
100% |
|
Marks |
1997 |
Retrospective parallel |
USA |
i: 14 / c: 19 |
Penetrating and Blunt |
100% |
100% |
|
Miles |
2004 |
Retrospective parallel |
USA |
i: 22/ c: 154 |
Penetrating |
100% |
100% |
|
Mutter |
1997 |
Retrospective parallel |
France |
i: 17 / c: 18 |
Abdominal stab wounds |
100% |
100% |
|
Obaid |
2021 |
Retrospective parallel |
USA |
i: 177 / c: 354 |
Traumatic diaphragamatic injury |
100% |
100% |
|
Omori |
2003 |
Retrospective pre/post |
Japan |
i: 11 / c: 13 |
Blunt |
100% |
100% |
|
Shams en Elaysi |
2021 |
Retrospective parallel |
Iran |
i:18 / c: 22 |
Penetrating |
100% |
100% |
|
Trejo-Avila |
2017 |
Retrospective parallel |
Mexico |
i: 19 / c: 19 |
Penetrating and Blunt |
100% |
100% |
HD = hemodynamic; I = intervention (laparoscopy); C = control (laparotomy)
Observational studies
Alzarouni (2022) performed a retrospective cohort study on the role of laparoscopy in abdominal trauma. Medical records were used from patients presenting with abdominal trauma in a level-I trauma centre in the United Arab Emirates. Records from adult patients (> 18 years), hemodynamically stable, with blunt or penetrating abdominal trauma requiring abdominal surgical intervention were included (n = 154). Patients with persistent hypotension, unresponsive to fluid resuscitation were excluded from this study. Mean age of the study population was 32.4 years, 90.9% was male and 63.6% had blunt trauma. Other baseline characteristics are presented in Table 2. In blunt abdominal trauma, a CT-scan was performed for every hemodynamically stable patient after fluid resuscitation and FAST examination. In penetrating abdominal trauma, the decision for surgical intervention depended on the clinical examination of each individual patient, regardless of the CT-scan evaluation. Initially, 57 patients underwent laparoscopy, and 97 patients underwent laparotomy. Of the 57 patients undergoing initial laparoscopy, 18 patients were converted to laparotomy. Outcomes included missed injuries and complications. Moreover, it was reported whether laparoscopy and laparotomy were therapeutic or non-therapeutic. There was no correction for confounding variables.
Elkbuli (2022) performed a retrospective cohort study with 1:1 propensity matching to compare patient outcomes between laparoscopy and laparotomy approaches in patients with single penetrating left upper quadrant injuries. Data from the American College of Surgeons (ACS) Trauma Quality Program (TQP) Participant Use File (PUF), including data from 700+ American Trauma centres was used. Patients aged 18 – 90 with single penetrating injuries to the left upper quadrant and/or left hemithorax who received laparoscopy or laparotomy were included for analysis. Patients who were dead on arrival, and patients with sustained traumatic brain injuries, blunt injuries, or two or more gun or stab wounds were excluded from the analysis. Patients in the laparoscopy (n = 486) and laparotomy (n = 486) group were matched using the following variables: age, gender, race, insurance status, injury type, injury severity score (ISS), comorbidities, trauma center level, and hospital bed size. The baseline variables appeared to be equally distributed across both groups, see Table 2. Both hemodynamically stable and hemodynamically unstable patients were included. The indications for either laparoscopy or laparotomy were not reported. Of the total study population, 2.4% underwent laparoscopy to laparotomy conversion, these patients were included in the laparotomy group.
Gomez (2022) performed a retrospective cohort study to investigate the feasibility and safety of laparoscopy in the treatment of stable penetrating abdominal trauma in a limited resources environment. Hospital records of patients presenting with stable penetrating abdominal trauma at a Colombian hospital were selected (n = 52). Patients younger than 16 years, patients with other body parts injuries and patients that had undergone successful non-operative management were excluded from the analysis. Indications for laparoscopy or laparotomy were not reported. Laparoscopy encompassed diagnostic laparoscopy, assisted laparoscopy and fully therapeutic laparoscopy. In the laparoscopy group, all patients were hemodynamically stable. In the laparotomy group, 75.4% of the patients was hemodynamically stable, see Table 2. Two patients from the laparoscopy group converted to laparotomy. Missed injuries, mortality, reintervention, complications, and conversion to laparotomy were reported as outcomes. There was no correction for confounding variables.
Table 2: baseline characteristics of the observational studies
|
Author |
Year |
Study design |
Country |
N (intervention/ control) |
Type of injury |
HD stable (intervention/ control) |
Extravasation (intervention/ control) |
|
Alzarouni |
2022 |
Retrospective cohort |
UAE |
i: 57 / c: 97 |
Blunt (38%) and penetrating (62%)
|
i: 100% / c: 100% |
Free air – i: 4 / c: 12 Free fluid – i: 7 / c: 1
|
|
Elkbuli |
2022 |
Retrospective propensity matched |
US (multicentre) |
i: 486 / c: 486 |
Single penetrating injuries to the left upper quadrant and/or left hemithorax |
i: 58.2% / c: 55.8% |
Not reported |
|
Gomez |
2022 |
Retrospective cohort |
Colombia (limited resources environment) |
i: 26 / c: 26 |
Stable penetrating abdominal trauma without other body parts injuries |
i: 100% / c: 75.4% |
Not reported |
HD = hemodynamic; I = intervention (laparoscopy); C = control (laparotomy)
Results
Missed injuries
Nineteen studies included in the review from Wang (2022) reported the outcome missed injuries. These results were pooled in a meta-analysis. The majority of studies did not report any missed injuries in the laparoscopy or laparotomy group. The pooled number of missed injuries in the laparoscopy group was 13/2524 (0.5%), compared to 46/2805 (1.6%) of the patients undergoing laparotomy. The pooled Risk Difference (RD) was -0.00 (95% CI -0.00 to 0.00), see Figure 1.
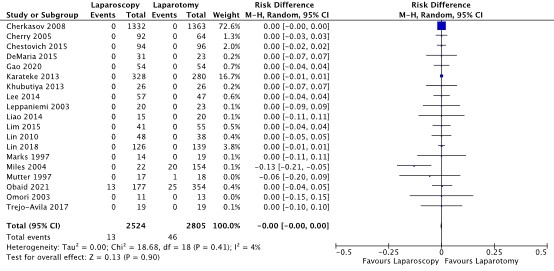
Figure 1. Forest plot showing the comparison between laparoscopy and laparotomy for the outcome missed injuries. Pooled risk difference, random effects model. Z: p-value of overall effect; df: degrees of freedom; SD: standard deviation; I2; statistical heterogeneity; CI: confidence interval.
Alzarouni (2022) and Gomez (2022) also reported missed injuries, however in both studies only information about missed injuries in the laparoscopy group. As a consequence, a Risk Ratio (RR) or RD could not be calculated. Both studies reported no missed injuries in the patients undergoing laparoscopy (n = 57 and n = 26 respectively)
Mortality
Twenty studies included in the review from Wang (2022) and Gomez (2022) reported the outcome mortality. These results were pooled in a meta-analysis. The majority of studies did not report mortality cases in the laparoscopy or laparotomy group. The pooled mortality rate in the laparoscopy group was 123/2169 (5.7%), compared to 213/2572 (8.3%) of the patients undergoing laparotomy. The pooled Risk Difference (RD) was -0.01 (95% CI: -0.03 to 0.00), see Figure 2.
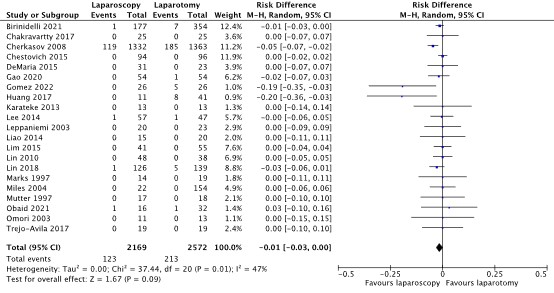
Figure 2. Forest plot showing the comparison between laparoscopy and laparotomy for the outcome mortality. Pooled risk difference, random effects model. Z: p-value of overall effect; df: degrees of freedom; SD: standard deviation; I2; statistical heterogeneity; CI: confidence interval.
Elkbuli (2022) calculated an adjusted Odds Ratio (OR) for mortality after matching patients in the laparoscopy group with patients in the laparotomy on multiple variables. In the laparoscopy group 1.2% mortality was reported, compared to 2.9% in the laparotomy group. The adjusted OR was 2.92 (95% CI: 0.32 to 26.31).
Reintervention
Five studies included in the review from Wang (2022) reported the outcome reintervention. In these studies re-intervention was defined as non-planned re-exploration. The results were pooled in a meta-analysis. The pooled number of reinterventions in the laparoscopy group was 2/470 (0.4%), compared to 16/660 (2.4%) of the patients undergoing laparotomy. The pooled RD was -0.01 (95% CI: -0.03 to 0.01), see Figure 3.

Figure 3. Forest plot showing the comparison between laparoscopy and laparotomy for the outcome reintervention. Pooled risk difference, random effects model. Z: p-value of overall effect; df: degrees of freedom; SD: standard deviation; I2; statistical heterogeneity; CI: confidence interval.
Gomez (2022) stated that “no reintervention (…) was reported” in the laparoscopy group. Data on reintervention rates in the laparotomy group was not reported.
Complications
Overall complications
Three studies (Alzarouni, 2022; Elkbuli, 2022, Gomez 2022) reported overall complication rates for the laparoscopy and laparotomy group, see Table 3. In Alzarouni (2022), complications were classified as surgical site infections, pulmonary complications, urinary tract infections, intra-abdominal collection and others. In Elkbuli (2022) and Gomez (2022) complications were not specified.
Table 3: resuts for the outcome complications (overall complication rate)
|
|
Laparoscopy |
Laparotomy |
Effect measure |
|
Alzarouni (2022) |
3/ 39 (7.7%) |
27 / 115 (23.5%) |
RD: -0.16 (95% CI: -0.27 to -0.04)
|
|
Elkbuli (2022) |
1.2% |
7.0% |
adjusted OR: 9.61 (1.94 to 47.48) *laparotomy (intervention) versus laparoscopy (control) |
|
Gomez (2022) |
1 (3.8%) |
1 (3.8%) |
RD: 0.00 (95% CI: -0.10 to 0.10)
|
RD = Risk Difference; CI = confidence interval; OR = Odds Ratio
In the review from Wang (2022) sub-analyses were made for different types of complications: wound infections, intra-abdominal abcess, pneumonia and bowel obstruction or ileus.
Wound infection
Seventeen studies included in the review from Wang (2022) reported the outcome wound infection These results were pooled in a meta-analysis. The pooled number of wound infection cases in the laparoscopy group was 52/2055 (2.5%), compared to 117/2416 (4.8%) of the patients undergoing laparotomy. The pooled RD was -0.03 (95% CI: -0.06 to -0.01), see Figure 4.
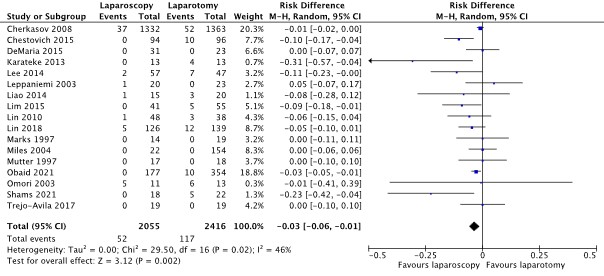
Figure 4. Forest plot showing the comparison between laparoscopy and laparotomy for the outcome wound infections (complication). Pooled risk difference, random effects model. Z: p-value of overall effect; df: degrees of freedom; SD: standard deviation; I2; statistical heterogeneity; CI: confidence interval.
Intra-abdominal abcess
Fifteen studies included in the review from Wang (2022) reported the outcome pneumonia. These results were pooled in a meta-analysis. The pooled number of cases of intra-abdominal abcess in the laparoscopy group was 7/595 (1.2%), compared to 14/744 (1.8%) of the patients undergoing laparotomy. The pooled RD was -0.00 (95% CI: -0.02 to 0.01), see Figure 5.
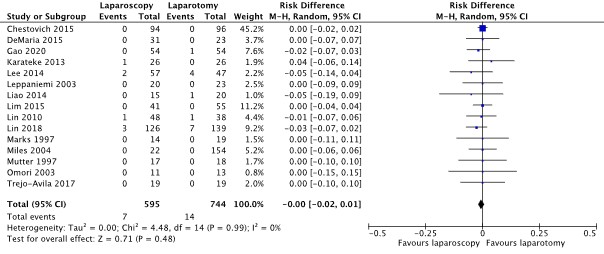
Figure 5. Forest plot showing the comparison between laparoscopy and laparotomy for the outcome intra-abdominal abcess (complication). Pooled risk difference, random effects model. Z: p-value of overall effect; df: degrees of freedom; SD: standard deviation; I2; statistical heterogeneity; CI: confidence interval.
Pneumonia
Twelve studies included in the review from Wang (2022) reported the outcome pneumonia. These results were pooled in a meta-analysis. The pooled number of pneumonia cases in the laparoscopy group was 17/1636 (1.0%), compared to 17/1799 (4.4%) of the patients undergoing laparotomy. The pooled RD was -0.03 (95% CI: -0.05 to -0.02), see Figure 6.
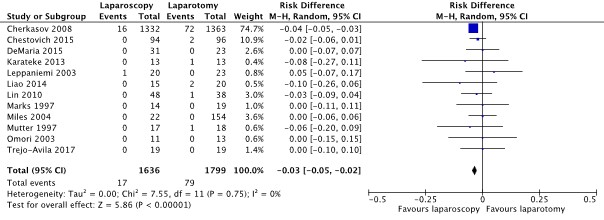
Figure 6. Forest plot showing the comparison between laparoscopy and laparotomy for the outcome pneumonia (complication). Pooled risk difference, random effects model. Z: p-value of overall effect; df: degrees of freedom; SD: standard deviation; I2; statistical heterogeneity; CI: confidence interval.
Bowel obstruction or ileus
Fourteen studies included in the review from Wang (2022) reported the outcome pneumonia. These results were pooled in a meta-analysis. The pooled number of bowel obstruction or ileus cases in the laparoscopy group was 9/1712 (0.5%), compared to 114/1880 (6%) of the patients undergoing laparotomy. The pooled RD was -0.03 (95% CI: -0.07 to -0.00), see Figure 7.
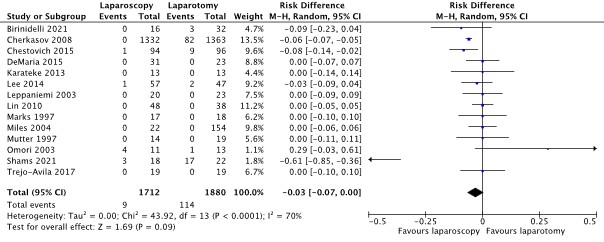
Figure 7. Forest plot showing the comparison between laparoscopy and laparotomy for the outcome bowel obstruction or ileus (complication). Pooled risk difference, random effects model. Z: p-value of overall effect; df: degrees of freedom; SD: standard deviation; I2; statistical heterogeneity; CI: confidence interval.
Quality of life
None of the studies reported the outcome ‘quality of life’.
Conversion (from laparoscopy to laparotomy)
The majority of studies reported conversion from laparoscopy to laparotomy. As this outcome measure only applies to the laparoscopy group, a comparative analysis could not be made and the GRADE-approach could not be applied. Nevertheless, the guideline development group considered these data relevant for this guideline. Wang (2022) reported that the average rate of conversion from laparoscopy to laparotomy was 25% (range: 0 – 45.1%). The data is presented below.
Table 3: laparoscopy to laparotomy conversion as reported in the included studies.
|
Author |
Year |
Conversion n (%) |
|
Alzarouni |
2022 |
18 (31.6%) |
|
Birinidelli (Wang 2022) |
2021 |
3 (19%) |
|
Chakravartty (Wang 2022) |
2017 |
1 (4%) |
|
Cherkasov (Wang 2022) |
2008 |
356 (26.7%) |
|
Cherry (Wang 2022) |
2005 |
36 (39.1%) |
|
Chestovich (Wang 2022) |
2015 |
15 (16%) |
|
DeMaria (Wang 2022) |
2000 |
14 (45.1%) |
|
Elkbuli |
2022 |
2.4% |
|
Gao (Wang 2022) |
2020 |
4 (7.4%) |
|
Gomez |
2022 |
2 (7.7%) |
|
Huang (Wang 2022) |
2017 |
0 (0%) |
|
Karateke (Wang 2022) |
2013 |
9 (34.6%) |
|
Khubutiya (Wang 2022) |
2013 |
130 (37.3%) |
|
Lee (Wang 2022) |
2014 |
2 (3.5%) |
|
Leppaniemi and Haapiainen (Wang 2022) |
2003 |
9 (45%) |
|
Liao (Wang 2022) |
2014 |
1 (6.7%) |
|
Lim (Wang 2022) |
2015 |
9 (18%) |
|
Lin (Wang 2022) |
2018 |
9 (7.1%) |
|
Lin (Wang 2022) |
2010 |
1 (2.1%) |
|
Marks (Wang 2022) |
1997 |
4 (28.6%) |
|
Miles (Wang 2022) |
2004 |
9 (40.9%) |
|
Mutter (Wang 2022) |
1997 |
4 (23.6%) |
|
Obaid (Wang 2022) |
2021 |
13 (7.3%) |
|
Omori (Wang 2022) |
2003 |
1 (9.1%) |
|
Shams en Elaysi (Wang 2022) |
2021 |
Not reported |
|
Trejo-Avila (Wang 2022) |
2017 |
1 (5.3%) |
Level of evidence of the literature
The level of evidence regarding the outcome measure missed injuries was retrieved from observational studies and therefore started ‘low’. The level of evidence was downgraded by one level because of study limitations including lack of adequate correction for confounding factors (-1 risk of bias). The final level of evidence was ‘very low’.
The level of evidence regarding the outcome measure mortality was retrieved from observational studies and therefore started ‘low’. The level of evidence was downgraded by one level because of study limitations including lack of adequate correction for confounding factors (-1 risk of bias). The final level of evidence was ‘very low’.
The level of evidence regarding the outcome measure reintervention was retrieved from observational studies and therefore started ‘low’. The level of evidence was downgraded by two levels because of study limitations including lack of adequate correction for confounding factors (-1 risk of bias) and the wise 95% confidence intervals, crossing the thresholds of minimal clinically (patients) important difference (-1 imprecision). The final level of evidence was ‘very low’.
The level of evidence regarding the outcome measure complications was retrieved from observational studies and therefore started ‘low’. The level of evidence was downgraded by one level because of study limitations including lack of adequate correction for confounding factors (-1 risk of bias). The final level of evidence was ‘very low’.
The level of evidence regarding the outcome measure ‘quality of life’ was not graded as it was not reported in the included studies.
The level of evidence regarding the outcome measure ‘conversion’ was not graded as it was not possible to make a comparison between the intervention (laparoscopy) and control (laparotomy)
A systematic review of the literature was performed to answer the following question:
What are the risks and benefits laparoscopy compared to laparotomy in patients with traumatic abdominal injury?
P = patients with traumatic abdominal injury
I = laparoscopy
C = laparotomy
O = missed injuries, mortality, conversion, re-intervention, complications, quality of life
Relevant outcome measures
The guideline development group considered missed injuries and mortality as a critical outcome measure for decision making; and conversion, reintervention, complications and quality of life as an important outcome measure for decision making.
A priori, the guideline development group did not define the outcome measures listed above but used the definitions used in the studies.
The guideline development group defined a relative risk (RR) of <0.90 and >1.10 and a risk difference (RD) of 10% as a minimal clinically (patient) important difference for the outcomes mortality and missed injuries. For the outcomes reintervention and complications a threshold of 25% was set as a minimal clinically (patient) important difference (0.80 < RR > 1.25 and RD 25%) set as a minimal clinically (patient) important difference. For quality of life (continuous outcome) a difference of 20% was considered clinically important.
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms until February 26, 2023. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 1476 hits. Studies were selected based on the following criteria: systematic reviews, randomized controlled trials and comparative observational studies comparing laparoscopy with laparotomy for the treatment of abdominal trauma. Seventeen studies were initially selected based on title and abstract screening. After reading the full text, twelve studies were excluded (see the table with reasons for exclusion under the tab Methods), and five studies were included.
Results
One systematic review and four observational studies were included in the analysis of the literature. Important study characteristics and results are summarized in the evidence tables. The assessment of the risk of bias is summarized in the risk of bias tables.
- Alzarouni, Noura, et al. "Role of laparoscopy in patients with abdominal trauma: Rashid Hospital Trauma Center experience." Journal of Emergency Medicine, Trauma & Acute Care 2022.5 (2022): 30.
- Cirocchi R, Fearnhead N, Vettoretto N, Cassini D, Popivanov G, Henry BM, Tomaszewski K, D'Andrea V, Davies J, Di Saverio S. The role of emergency laparoscopic colectomy for complicated sigmoid diverticulits: A systematic review and meta-analysis. Surgeon. 2019 Dec;17(6):360-369. doi: 10.1016/j.surge.2018.08.010. Epub 2018 Oct 9. PMID: 30314956.
- Elkbuli A, Andrade R, Ngatuvai M, Khan A, Liu H, Bilski T, Ang D. Assessment of Outcomes in Laparotomy vs Laparoscopy: A Propensity Score Matched Analysis of Patients Sustaining Single Penetrating Left Upper Quadrant Injury. Am Surg. 2022 Dec 16:31348221146969. doi: 10.1177/00031348221146969. Epub ahead of print. PMID: 36526271.
- Gómez EJI, Vargas LFC, Lozada-Martinez ID, Reyes M, Pedraza M, Forero N, Guardo-Carmona D, Narvaez-Rojas AR. Laparoscopy has better performance than laparotomy in the treatment of stable penetrating abdominal trauma: A retrospective cross-sectional study in a trauma referral hospital in Colombia. Health Sci Rep. 2022 May 24;5(3):e640. doi: 10.1002/hsr2.640. PMID: 35620533; PMCID: PMC9128394.
- Sermonesi G, Tian BWCA, Vallicelli C, Abu-Zidan FM, Damaskos D, Kelly MD, Leppäniemi A, Galante JM, Tan E, Kirkpatrick AW, Khokha V, Romeo OM, Chirica M, Pikoulis M, Litvin A, Shelat VG, Sakakushev B, Wani I, Sall I, Fugazzola P, Cicuttin E, Toro A, Amico F, Mas FD, De Simone B, Sugrue M, Bonavina L, Campanelli G, Carcoforo P, Cobianchi L, Coccolini F, Chiarugi M, Di Carlo I, Di Saverio S, Podda M, Pisano M, Sartelli M, Testini M, Fette A, Rizoli S, Picetti E, Weber D, Latifi R, Kluger Y, Balogh ZJ, Biffl W, Jeekel H, Civil I, Hecker A, Ansaloni L, Bravi F, Agnoletti V, Beka SG, Moore EE, Catena F. Cesena guidelines: WSES consensus statement on laparoscopic-first approach to general surgery emergencies and abdominal trauma. World J Emerg Surg. 2023 Dec 8;18(1):57. doi: 10.1186/s13017-023-00520-9. PMID: 38066631; PMCID: PMC10704840.
- Smyth L, Bendinelli C, Lee N, Reeds MG, Loh EJ, Amico F, Balogh ZJ, Di Saverio S, Weber D, Ten Broek RP, Abu-Zidan FM, Campanelli G, Beka SG, Chiarugi M, Shelat VG, Tan E, Moore E, Bonavina L, Latifi R, Hecker A, Khan J, Coimbra R, Tebala GD, Søreide K, Wani I, Inaba K, Kirkpatrick AW, Koike K, Sganga G, Biffl WL, Chiara O, Scalea TM, Fraga GP, Peitzman AB, Catena F. WSES guidelines on blunt and penetrating bowel injury: diagnosis, investigations, and treatment. World J Emerg Surg. 2022 Mar 4;17(1):13. doi: 10.1186/s13017-022-00418-y. PMID: 35246190; PMCID: PMC8896237.
- Wang J, Cheng L, Liu J, Zhang B, Wang W, Zhu W, Guo Y, Bao C, Hu Y, Qi S, Wang K, Zhao S. Laparoscopy vs. Laparotomy for the Management of Abdominal Trauma: A Systematic Review and Meta-Analysis. Front Surg. 2022 Mar 8;9:817134. doi: 10.3389/fsurg.2022.817134. PMID: 35350141; PMCID: PMC8957831.
Evidence table for systematic review of RCTs and observational studies (intervention studies)
|
Study reference |
Study characteristics |
Patient characteristics |
Intervention (I) |
Comparison / control (C)
|
Follow-up |
Outcome measures and effect size |
Comments |
|
Wang, 2022
Study characteristics and results are extracted from the SR (unless stated otherwise) |
SR and meta-analysis of RCTs and observational studies
Literature search up to June, 2021
a: Birinidelli, 2021 b: Chakravartty, 2017 c: Cherkasov, 2008 d: Cherry, 2005 e: Chestovich, 2015 f: DeMaria, 2000 g: Gao, 2020 h: Huang, 2017 i: Karateke, 2013 j: Khubutiya, 2013 k: Lee, 2014 l: Leppaniem and Haapiainen, 2003 m: Liao, 2014 n: Lim, 2015 o: Lin, 2018 p: Lin, 2010 q: Marks, 1997 r: Miles, 2004 s: Mutter, 1997 t: Obaid, 2021 u: Omori, 2003 v: Shams en Elaysi, 2021 w: Trejo-Avila, 2017
Study design: RCT: l Prospective observational: f, i Retrospective pre-post observational: c, k, p, u Retrospective parallel observational:a, b, d, e, g, h, j, m, n, o, q, r, s, t, v, w.
Setting and Country: a: Italy b: UK c: Russia d:USA e: USA f: USA g: China h: USA i: Turkey j: Russia k: Taiwan l: Finalnd m: Taiwan n: South Korea o: Taiwan p: Taiwan q: USA r: USA s: France t: USA u: Japan v: Iran w: Mexico
Source of funding and conflicts of interest: Of systematic review: none
|
Inclusion criteria SR: - comparative studies comparing laparoscopy and laparotomy for the management of abdominal trauma - studies in English
Exclusion criteria SR: - studies in children (age < 18 years)
23 studies included
Important patient characteristics at baseline:
N, mean age a: i: 16 / c: 22; Splenic trauma () b: i: 25 / c: 25; Abdominal trauma () c: i: 1332 / c: 1363; Penetrating () d: i: 92/ c: 64; Penetrating () e: i: 94 / c: 96; Penetrating () f: i: 31 / c: 23; Abdominal stab wounds () g: i: 54 / c: 54; Penetrating and Blunt () h: i: 11 / c: 41; Blunt () i: i: 26 / c: 26; Penetrating () j: i: 328 / c: 280; Penetrating and Blunt () k: i: 57 / c: 47; Blunt () l: i: 20 / c: 23; Stab wounds () m: i: 15 / c:22; Penetrating and Blunt () n: i: 41 / c: 55; Abdominal trauma () o: i: 126 / c: 139; Blunt () p: i: 48 / c: 38; stab wounds () q: i: 14 / c: 19; Penetrating and Blunt () r: i: 22/ c: 154; Penetrating () s: i: 17 / c: 18; Abdominal stab wounds () t: i: 177 / c: 354; Traumatic diaphragamatic injury () u: i: 11 / c: 13; Blunt () v: i:18 / c: 22; Penetrating () w: i: 19 / c: 19; Penetrating and Blunt ()
Groups comparable at baseline? Not clear |
Laparoscopy
|
Laparotomy |
Not reported
|
Outcome measure-1: Conversion: n (%) a: 3 (19%) b: 1 (4%) c: 356 (26.7%) d: 36 (39.1%) e: 15 (16%) f: 14 (45.1%) g: 4 (7.4%) h: 0 (0%) i: 9 (34.6%) j: 130 (37.3%) k: 2 (3.5%) l: 9 (45%) m: 1 (6.7%) n: 9 (18%) o: 9 (7.1%) p: 1 (2.1%) q: 4 (28.6%) r: 9 (40.9%) s: 4 (23.6%) t: 13 (7.3%) u: 1 (9.1%) v: Not reported w: 1 (5.3%)
Outcome measure-2: missed injury Pooled effect: I: n = 13 / 2524 C: n = 46 / 2805 RD = 0.00 (0.00 to 0.00) (for outcomes reported in individual studies, see forest plot or Wang 2022)
Outcome measure-3: Mortality Pooled effect: I: n = 123 / 2143 C: n = 208 / 2546 RD = -0.01 (-0.03 to 0.00) (for outcomes reported in individual studies, see forest plot or Wang 2022)
Outcome measure-4: complications wound infection I: n = 52 / 2055 C: n = 117 / 2416 RD = -0.03 (-0.06 to -0.01)
Pooled effect: (for outcomes reported in individual studies, see forest plot or Wang 2022.)
Outcome measure-4: complications re-operation I: n = 2 / 470 C: n = 16 / 660 RD = -0.01 (-0.03 to 0.01)
Pooled effect: (for outcomes reported in individual studies, see forest plot or Wang 2022.)
|
Facultative: “The author’s concluded that: laparoscopic surgery is a reasonable alternative to open surgery for the appropriate patients, but the intervention should be performed by experienced surgeons in well-equipped health care facilities”
Subgroup analyses were performed. These subgroup analysis did not show any statistical difference between subgroups based on study design, injury mechanism, and the purpose of laparoscopy use for primary outcomes. The pooled results of high-quality studies were consistent with the results of the primary analyses for all outcomes (except pneumonia) |
Evidence table for intervention studies (randomized controlled trials and non-randomized observational studies [cohort studies, case-control studies, case series])1
|
Study reference |
Study characteristics |
Patient characteristics 2 |
Intervention (I) |
Comparison / control (C) 3
|
Follow-up |
Outcome measures and effect size 4 |
Comments |
|
Alzarouni 2022 |
Type of study: Retrospective cohort study
Setting and country: Level-I trauma centre, United Arab Emirates 2016 - 2018
Funding and conflicts of interest: Not reported |
Inclusion criteria: - Adults > 18 years - Hemodynamically stable or responder patients - all patients who underwent surgical intervention
Exclusion criteria: Patients with persistent hypotension unresponsive to fluid resuscitation were excluded from this study
N total at baseline: Intervention: 57 Control: 97
Important prognostic factors2: Mean age: 32.4 years, 90.9% male
Groups comparable at baseline? Probably no
|
Laparoscopy
|
Laparotomy (open exploration)
|
Length of follow-up: n.a.
Loss-to-follow-up: Medical records with incomplete documentation were excluded
|
Outcome measures and effect size (include 95%CI and p-value if available):
Missed injuries i: 0/57 c: not reported
Complications i: 3/ 39 (7.7%) c: 27 / 115 (23.5%)
Conversion i: 18/57 (31.6%) |
The author’s concluded that: “Using laparoscopy in trauma is associated with a low rate of missed diagnostic intent and can reduce unnecessary laparotomies with all associated complications” It was reported that the percentage of ‘unnecessary’ (or non-therapeutic) laparotomy was’ 18.2% (21/115 cases)
|
|
Elkbuli 2022 |
Type of study: Propensity-matched Retrospective cohort study
Setting and country: Data from ACS-TQP-PUF database -encompassing 700 trauma centres in the US Between 2016 and 2019
Funding and conflicts of interest: Not reported
|
Inclusion criteria: - Adult trauma patients aged 18 – 90 Exclusion criteria: - patients pronounced dead on arrival - patients with sustained traumatic brain injuries, blunt injuries, or two or more gunshot or stabwounds
N total at baseline: Intervention: 486 Control: 486
Important prognostic factors2: Age was equally distributed across groups
% male I: 80% C: 84%
HD stable I: 58.2% C: 55.8%
Groups comparable at baseline? Probably yes |
Laparoscopy |
laparotomy |
Length of follow-up: n.a.
Loss-to-follow-up: n.a.
|
Outcome measures and effect size (include 95%CI and p-value if available):
Inpatient mortality i: 1.2% c: 2.9% adjusted OR: 2.92 (0.32 to 26.31) à laparotomy versus laparoscopy
Complication rates i: 1.2% c: 7.0% adjusted OR: 9.61 (1.94 to 47.48) à laparotomy versus laparoscopy
|
Stratification of each cohort was based on the following variables: hemodynamic stability (hemodynamically stable defined as heart rate (HR) < 100 beats per minute and systolic blood pressure (SBP) ≥90 mmHg and hemodynamically unstable defined as HR ≥100 and SBP <90), BMI (Underweight: <18.5, Normal: 18.5-24.9, Overweight: 25-29.9, Obese: 30-39.9, Morbidly Obese: ≥40), and mechanism of injury (gunshot wound, knife wound, or other non-ballistic penetrating object wound).
2.4% of all patients underwent laparoscopy to laparotomy conversion; these patients were included in the laparotomy cohort. |
|
Gomez 2022 |
Type of study: Retrospective Cross-sectional study
Setting and country: single-centre, Colombia
Funding and conflicts of interest: None
|
Inclusion criteria: - all adults stable penetrating abdominal trauma patients approached with laparoscopy and laparotomy
Exclusion criteria: - patients younger than 16 years - patients with other body parts injuries - those who had undergone successful nonoperative management
N total at baseline: Intervention: 26 Control: 26
Important prognostic factors2: HD stable I: 0 (0%) C: 9 (34.6%)
Groups comparable at baseline? Probably no |
Laparoscopy |
Laparotomy |
Length of follow-up: n.a.
Loss-to-follow-up: Cases with missing records were excluded from the study
|
Outcome measures and effect size (include 95%CI and p-value if available):
Missed injuries: “no missed injuries were reported”
Mortality i: 0 (0) c: 5 (19.2%)
reintervention “no reintervention (…) was reported”
Complication i: 1 (3.8%) c: 1 (3.8%)
Conversion to laparotomy: 2 (7.7%)
|
The author’s concluded that: “Surgical results in this study found a safe scenario in a limited resources environment for the application of the laparoscopic technique to approach penetrating abdominal trauma in stable patients without missed injuries, low threshold of conversion to open approach, and additionally not presenting a higher percentage of complications compared to the laparotomy group”
|
|
|
|
|
|
|
|
|
|
Risk of bias table for interventions studies (cohort studies based on risk of bias tool by the CLARITY Group at McMaster University)
|
Author, year |
Selection of participants
Was selection of exposed and non-exposed cohorts drawn from the same population?
|
Exposure
Can we be confident in the assessment of exposure?
|
Outcome of interest
Can we be confident that the outcome of interest was not present at start of study?
|
Confounding-assessment
Can we be confident in the assessment of confounding factors? |
Confounding-analysis
Did the study match exposed and unexposed for all variables that are associated with the outcome of interest or did the statistical analysis adjust for these confounding variables? |
Assessment of outcome
Can we be confident in the assessment of outcome?
|
Follow up
Was the follow up of cohorts adequate? In particular, was outcome data complete or imputed? |
Co-interventions
Were co-interventions similar between groups?
|
Overall Risk of bias
|
|
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Definitely yes, probably yes, probably no, definitely no |
Low, Some concerns, High |
|
|
Alzarouni 2022 |
Definitely yes
Reason: participants were selected from the same hospital database |
Definitely yes
Reason: based on hospital records
|
Definitely yes
Reason: all outcomes took place after the intervention was executed
|
Definitely yes
Reason: variables retrieved from hospital records
|
Definitely no
Reason: no correction for confounding variables
|
Definitely yes
Reason: retrieved from hospital data
|
No information
A retrospective design was used
|
No information
|
High for all outcomes Due to the lack of correction for confounding factors |
|
Elkbuli 2022 |
Definitely yes
Reason: participants were selected from the same hospital database |
Definitely yes
Reason: based on hospital records
|
Definitely yes
Reason: all outcomes took place after the intervention was executed
|
Definitely yes
Reason: variables retrieved from hospital records
|
Probably yes:
Reason: propensity-matching and multivariate analysis with confounding variables was executed
|
Definitely yes
Reason: retrieved from hospital data
|
No information
A retrospective design was used
|
No information
|
Low for all outcomes |
|
Gomez 2022 |
Definitely yes
Reason: participants were selected from the same hospital database |
Definitely yes
Reason: based on hospital records
|
Definitely yes
Reason: all outcomes took place after the intervention was executed
|
Definitely yes
Reason: variables retrieved from hospital records
|
Definitely no
Reason: no correction for confounding variables
|
Definitely yes
Reason: retrieved from hospital data
|
No information
A retrospective design was used
|
No information
|
High for all outcomes Due to the lack of correction for confounding factors |
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Elkbuli A, Newsome K, Fanfan D, Sutherland M, Bilski T, Liu H, Ang D. Laparoscopic Versus Laparotomy Surgical Interventions for Trauma Patients With Single Upper Left Quadrant Penetrating Injuries: Analysis of the American College of Surgeons Trauma Quality Improvement Program Dataset. Am Surg. 2022 Sep;88(9):2182-2193. doi: 10.1177/00031348221101510. Epub 2022 May 19. PMID: 35592893. |
Same study population as Elkbuli (2022). Lower quality study (the other trial did propensity matching) |
|
Kumar R, Mishra A, Damde H, Yadav P, Yadav SK. Access, Safety, and Barriers in Adoption of Emergency Laparoscopy Surgery for Trauma Patients in a Low-Resource Setting. Surg J (N Y). 2023 Mar 3;9(1):e58-e61. doi: 10.1055/s-0043-1761951. PMID: 36873295; PMCID: PMC9984267. |
Study executed in low resource setting, not applicable to Dutch hospital setting |
|
Lin HF, Chen YD, Lin KL, Wu MC, Wu CY, Chen SC. Laparoscopy decreases the laparotomy rate for hemodynamically stable patients with blunt hollow viscus and mesenteric injuries. Am J Surg. 2015 Aug;210(2):326-33. doi: 10.1016/j.amjsurg.2014.11.009. Epub 2015 Apr 14. PMID: 25963637. |
Publication date before Wang (2022) |
|
Nicolau AE. Is laparoscopy still needed in blunt abdominal trauma? Chirurgia (Bucur). 2011 Jan-Feb;106(1):59-66. PMID: 21520776. |
More recent and higher quality SR available (Wang 2022) |
|
Li Y, Xiang Y, Wu N, Wu L, Yu Z, Zhang M, Wang M, Jiang J, Li Y. A Comparison of Laparoscopy and Laparotomy for the Management of Abdominal Trauma: A Systematic Review and Meta-analysis. World J Surg. 2015 Dec;39(12):2862-71. doi: 10.1007/s00268-015-3212-4. PMID: 26316111. |
More recent and higher quality SR available (Wang 2022) |
|
Hajibandeh S, Hajibandeh S, Gumber AO, Wong CS. Laparoscopy versus laparotomy for the management of penetrating abdominal trauma: A systematic review and meta-analysis. Int J Surg. 2016 Oct;34:127-136. doi: 10.1016/j.ijsu.2016.08.524. Epub 2016 Aug 26. PMID: 27575832. |
More recent and higher quality SR available (Wang 2022) |
|
Marsden MER, Vulliamy PED, Carden R, Naumann DN, Davenport RA; National Trauma Research and Innovation Collaborative (NaTRIC). Trauma Laparotomy in the UK: A Prospective National Service Evaluation. J Am Coll Surg. 2021 Sep;233(3):383-394.e1. doi: 10.1016/j.jamcollsurg.2021.04.031. Epub 2021 May 17. PMID: 34015456. |
No comparison between laparoscopy and laparotomy |
|
Sitnikov V, Yakubu A, Sarkisyan V, Turbin M. The role of video-assisted laparoscopy in management of patients with small bowel injuries in abdominal trauma. Surg Endosc. 2009 Jan;23(1):125-9. doi: 10.1007/s00464-008-9910-3. Epub 2008 Apr 10. PMID: 18401644. |
No comparison between laparoscopy and laparotomy |
|
Cirocchi R, Birindelli A, Inaba K, Mandrioli M, Piccinini A, Tabola R, Carlini L, Tugnoli G, Di Saverio S. Laparoscopy for Trauma and the Changes in its Use From 1990 to 2016: A Current Systematic Review and Meta-Analysis. Surg Laparosc Endosc Percutan Tech. 2018 Feb;28(1):1-12. doi: 10.1097/SLE.0000000000000466. PMID: 28915204. |
More recent and higher quality SR available (Wang 2022) |
|
Ki YJ, Jo YG, Park YC, Kang WS. The Efficacy and Safety of Laparoscopy for Blunt Abdominal Trauma: A Systematic Review and Meta-Analysis. J Clin Med. 2021 Apr 24;10(9):1853. doi: 10.3390/jcm10091853. PMID: 33923206; PMCID: PMC8123164. |
More recent and higher quality SR available (Wang 2022) |
|
Cocco AM, Bhagvan S, Bouffler C, Hsu J. Diagnostic laparoscopy in penetrating abdominal trauma. ANZ J Surg. 2019 Apr;89(4):353-356. doi: 10.1111/ans.15140. Epub 2019 Mar 14. PMID: 30873735. |
Wrong outcome: study on diagnostic accuracy, does not report one of the predefined outcomes |
|
Arnold MR, Lu CD, Thomas BW, Sachdev G, Cunningham KW, Vaio R, Heniford BT, Sing RF. Advancing the Use of Laparoscopy in Trauma: Repair of Intraperitoneal Bladder Injuries. Am Surg. 2019 Dec 1;85(12):1402-1404. PMID: 31908226. |
Wrong outcome: study does not report one of the predefined outcomes |
|
Majewski W. Diagnostic laparoscopy for the acute abdomen and trauma. Surg Endosc. 2000 Oct;14(10):930-7. doi: 10.1007/s004640000197. PMID: 11080406. |
No comparison between laparoscopy and laparotomy, all patients receive laparoscopy |
Beoordelingsdatum en geldigheid
Publicatiedatum : 23-06-2025
Beoordeeld op geldigheid : 12-05-2025
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd uit de Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2022 een werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met abdominale letsels.
Werkgroep
- Mevr. dr. C.M. (Charlotte) Lameijer (voorzitter richtlijnwerkgroep); traumachirurg Amsterdam UMC, Nederlandse Vereniging voor Heelkunde (NVvH)
- Dhr. dr. E.A. (Erwin) Gorter; traumachirurg LUMC, Nederlandse Vereniging voor Heelkunde (NVvH)
- Dhr. dr. E.R. (Eric) Manusama; GI- en HPB-chirurg Medisch Centrum Leeuwarden, Nederlandse Vereniging voor Heelkunde (NVvH)
- Dhr. dr. R. (Rigo) Hoencamp; vaat- en traumachirurg, Ministerie van Defensie, Alrijne Ziekenhuis Leiderdorp, Nederlandse Vereniging voor Heelkunde (NVvH)
- Dhr. dr. O.J.F. (Oscar) van Waes; traumachirurg Erasmus MC, Nederlandse Vereniging voor Heelkunde (NVvH)
- Mevr. dr. D.C. (Dominique) Olthof; traumachirurg en chirurg bij kinderen, HagaZiekenhuis Den Haag, Nederlandse Vereniging voor Heelkunde (NVvH)
- Dhr. dr. R.W. (Rutger) van der Meer; interventieradioloog, LUMC, Nederlandse Vereniging voor Radiologie (NVvR)
- Mevr. drs. A. (Arezo) Mohamad; interventieradioloog, Erasmus MC en Groene Hart Ziekenhuis, Nederlandse Vereniging voor Radiologie (NVvR)
- Dhr. drs. T. (Teun) van den Heijkant; SEH-arts, Catharina Ziekenhuis Eindhoven, Nederlandse Vereniging van Spoedeisende Hulp Artsen (NVSHA)
Klankbordgroep
- Mevr. drs. A. (Anneke) Dijkman; gynaecoloog, Reinier de Graaf Gasthuis Delft, Nederlandse Vereniging voor Obstetrie en Gynaecologie (NVOG)
- Dhr. prof. dr. V.A. (Victor) de Ridder; kinderchirurg, UMC Utrecht, Nederlandse Vereniging voor Heelkunde (NVvH)
- Dhr. Prof. dr. R.J.A (Jeroen) van Moorselaar, uroloog, Amsterdam UMC, Nederlandse Vereniging voor Urologie (NVU)
- Mevr. dr. D.G. (Diana) Taekema, klinisch geriater, Rijnstate Ziekenhuis, Nederlandse Vereniging voor Klinische Geriatrie (NVKG)
- Mevr. K. (Klaartje) Spijkers, senior-adviseur patiëntenbelang, Patiëntenfederatie Nederland
Met ondersteuning van
- Mevr. dr. R. (Romy) Zwarts - van de Putte, adviseur, Kennisinstituut van Medisch Specialisten
- Mevr. MSc. D.G. (Dian) Ossendrijver, adviseur, Kennisinstituut van de Federatie Medisch Specialisten
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle werkgroepleden hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een module worden wijzigingen in belangen aan de voorzitter doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase.
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
|
Naam |
Functienaam en werkgever |
Nevenwerkzaamheden |
Persoonlijke Financiële Belangen |
Persoonlijke Relaties |
Extern gefinancierd onderzoek |
Intell. belangen en reputatie |
Overige belangen |
Actie |
|
Charlotte Lameijer (vz) |
Traumachirurg Werkgever: Amsterdam UMC |
Traumachirurg, onderwijs in polytrauma/bovenste extremiteitletsel, ATLS/DSATC instructeur
|
Geen |
Nee |
Geen |
Geen |
Geen |
Geen restrictie. |
|
Arezo Mohamad |
Interventieradioloog Werkgever: Erasmus MC en Groene Hart Ziekenhuis, |
Diagnostiek |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen restrictie. |
|
Dominique Olthof |
Trauma- en kinderchirurg |
|
Geen |
Geen |
Geen |
Geen |
Geen |
Geen restrictie |
|
Eric Manusama |
GI en HPB chirurg Werkgever: MCL Leeuwarden |
Bestuurslid van de vakgroep Militaire chirurgie |
Geen |
Geen |
Geen |
Geen i |
Geen |
Geen restrictie. |
|
Erwin Gorter |
Traumachirurg Werkgever: LUMC |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen restrictie. |
|
Rigo Hoencamp |
Chirurg Werkever: Alrijne |
Defensie |
Nee |
Nee |
Diverse onderzoekslijnen (acute bloedingen, resuscitatie, duurzaam inzetbaar (onderste extremiteit klachten). Dit onderzoek wordt gefinancierd door defensie en gerelateerde stichtingen (geen commerciële instellingen). |
Nee |
Nee |
Geen restrictie, geen commercieel gefinancierd onderzoek. |
|
Rutger van der Meer |
Interventieradioloog Werkgever: LUMC |
Secretaris Nederlandse Vereniging van Interventieradiologie, onbetaald |
Geen |
Nee |
Nvt |
Geen |
Geen |
Geen restrictie. |
|
Teun van den Heijkant |
SEH-arts KNMG Werkgever: Catharina Ziekenhuis Eindhoven |
Instructeur procedurele sedatie cursus; betaald |
Nee |
Geen |
Nee |
Nee |
Geen |
Geen restrictie. |
|
Oscar van Waes |
Traumachirurg Werkgever: Erasmus MC |
Defensie |
geen |
geen |
nvt |
nvt |
nvt |
Geen restrictie. |
|
Naam |
Functienaam en werkgever |
Nevenwerkzaamheden |
Persoonlijke Financiële Belangen |
Persoonlijke Relaties |
Extern gefinancierd onderzoek |
Intell. belangen en reputatie |
Overige belangen |
Actie |
|
Anneke Dijkman |
Gynaecoloog, Werkgever: Reinier de Graaf Gasthuis, Delft |
Bestuurslid MOET cursus van ALSG groep (geen betaalde functie; dus geen financiële belangen) |
Geen |
Geen |
Geen |
Geen (behoudens de kennis van de ALSG- MOET cursus) |
Geen |
Geen restrictie. |
|
Jeroen van Moorselaar |
Uroloog Werkgever: Amsterdam UMC |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen |
Geen restrictie; klankbordgroep |
|
Diana Taekema |
Klinisch geriater |
Opleider klinische geriatrie |
Geen |
Geen belang |
Ja |
Geen belang |
Geen |
Geen restrictie; klankbordgroep |
|
Klaartje Spijkers |
Senior Adviseur Patientenfederatie |
nvt |
nvt |
nvt |
nvt |
nvt |
nvt |
Geen restrictie; klankbordgroep |
|
Victor de Ridder |
Hoogleraar Utrechts Medisch Centrum, hoofd Emergency Care and Logistics, Trauma and Pediatric Trauma Werkgever: UMC Utrecht |
Editor Rockwood and Green Fractures in Adults en Fractures in Children |
Dienstverband UMC Utrecht |
geen |
geen |
geen |
geen |
Geen restrictie; klankbordgroep |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door het uitnodigen van Patiëntenfederatie Nederland (PFN) voor de schriftelijke knelpuntenanalyse en deelname van PFN aan de klankbordgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptrichtlijn is tevens voor commentaar voorgelegd aan Patiëntenfederatie Nederland en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule is conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uitgevoerd om te beoordelen of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema op de Richtlijnendatabase).
Module |
Uitkomst raming |
Toelichting |
|
Laparascopie |
geen financiële gevolgen |
Uit de toetsing volgt dat de aanbeveling(en) niet breed toepasbaar zijn (<5000 patiënten) en zal daarom naar verwachting geen substantiële financiële gevolgen hebben voor de collectieve uitgaven. |
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 2.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Knelpuntenanalyse en uitgangsvragen
Tijdens de voorbereidende fase inventariseerde de werkgroep de knelpunten in de zorg voor patiënten met abdominale letsels na trauma. Tevens zijn er knelpunten aangedragen door middel van een schriftelijke knelpuntenanalyse.
Op basis van de uitkomsten van de knelpuntenanalyse zijn door de werkgroep concept-uitgangsvragen opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvraag behorende bij de uitgangsvraag inventariseerde de werkgroep welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. Hierbij werd een maximum van acht uitkomstmaten gehanteerd. De werkgroep waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerde de werkgroep tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur is te vinden onder ‘Zoeken en selecteren’ onder Onderbouwing. Indien mogelijk werd de data uit verschillende studies gepoold in een random-effects model [Review Manager 5.4] werd gebruikt voor de statistische analyses. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie http://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding).
GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in richtlijnen volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE methodiek.
Formuleren van aanbevelingen
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door de werkgroep wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. De werkgroep heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
In de knelpuntenanalyse en bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen. Meer algemene, overkoepelende, of bijkomende aspecten van de organisatie van zorg worden behandeld in de module Organisatie van zorg.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd aan de betrokken (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd ter commentaar. De commentaren werden verzameld en besproken met de werkgroep. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door de werkgroep. De definitieve richtlijnmodule werd aan de deelnemende (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd voor autorisatie en door hen geautoriseerd dan wel geaccordeerd.
Literatuur
Agoritsas T, Merglen A, Heen AF, Kristiansen A, Neumann I, Brito JP, Brignardello-Petersen R, Alexander PE, Rind DM, Vandvik PO, Guyatt GH. UpToDate adherence to GRADE criteria for strong recommendations: an analytical survey. BMJ Open. 2017 Nov 16;7(11):e018593. doi: 10.1136/bmjopen-2017-018593. PubMed PMID: 29150475; PubMed Central PMCID: PMC5701989.
Alonso-Coello P, Schünemann HJ, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Rada G, Rosenbaum S, Morelli A, Guyatt GH, Oxman AD; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ. 2016 Jun 28;353:i2016. doi: 10.1136/bmj.i2016. PubMed PMID: 27353417.
Alonso-Coello P, Oxman AD, Moberg J, Brignardello-Petersen R, Akl EA, Davoli M, Treweek S, Mustafa RA, Vandvik PO, Meerpohl J, Guyatt GH, Schünemann HJ; GRADE Working Group. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 2: Clinical practice guidelines. BMJ. 2016 Jun 30;353:i2089. doi: 10.1136/bmj.i2089. PubMed PMID: 27365494.
Brouwers MC, Kho ME, Browman GP, Burgers JS, Cluzeau F, Feder G, Fervers B, Graham ID, Grimshaw J, Hanna SE, Littlejohns P, Makarski J, Zitzelsberger L; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010 Dec 14;182(18):E839-42. doi: 10.1503/cmaj.090449. Epub 2010 Jul 5. Review. PubMed PMID: 20603348; PubMed Central PMCID: PMC3001530.
Hultcrantz M, Rind D, Akl EA, Treweek S, Mustafa RA, Iorio A, Alper BS, Meerpohl JJ, Murad MH, Ansari MT, Katikireddi SV, Östlund P, Tranæus S, Christensen R, Gartlehner G, Brozek J, Izcovich A, Schünemann H, Guyatt G. The GRADE Working Group clarifies the construct of certainty of evidence. J Clin Epidemiol. 2017 Jul;87:4-13. doi: 10.1016/j.jclinepi.2017.05.006. Epub 2017 May 18. PubMed PMID: 28529184; PubMed Central PMCID: PMC6542664.
Medisch Specialistische Richtlijnen 2.0 (2012). Adviescommissie Richtlijnen van de Raad Kwalitieit. http://richtlijnendatabase.nl/over_deze_site/over_richtlijnontwikkeling.html
Neumann I, Santesso N, Akl EA, Rind DM, Vandvik PO, Alonso-Coello P, Agoritsas T, Mustafa RA, Alexander PE, Schünemann H, Guyatt GH. A guide for health professionals to interpret and use recommendations in guidelines developed with the GRADE approach. J Clin Epidemiol. 2016 Apr;72:45-55. doi: 10.1016/j.jclinepi.2015.11.017. Epub 2016 Jan 6. Review. PubMed PMID: 26772609.
Schünemann H, Brożek J, Guyatt G, et al. GRADE handbook for grading quality of evidence and strength of recommendations. Updated October 2013. The GRADE Working Group, 2013. Available from http://gdt.guidelinedevelopment.org/central_prod/_design/client/handbook/handbook.html.
Zoekverantwoording
Zoekverantwoording
Algemene informatie
|
Richtlijn: Abdominale letsels na trauma |
|
|
Uitgangsvraag: Wat is de rol van laparoscopie bij patiënten met abdominaal letsel na trauma? |
|
|
Database(s): Embase.com, Medline(Ovid) |
Datum: |
|
Periode: n.v.t. |
Talen: nvt |
|
Literatuurspecialist: Eugenie Delvaux |
|
|
BMI zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Bij gebruikmaking van een volledig zoekblok zal naar de betreffende link op de website worden verwezen. |
|
|
Toelichting en opmerkingen:
Er is gezocht met de volgende elementen: Abdominal injury/trauma EN laparoscopie EN laparatomie.
Alle sleutelartikelen worden gevonden.
|
|
Zoekopbrengst
|
|
EMBASE |
OVID/Medline |
Ontdubbeld |
|
SRs |
138 |
46 |
145 |
|
RCTs |
111 |
60 |
112 |
|
OBS |
1300 |
357 |
1219 |
|
Totaal |
|
|
1476 |
Zoekstrategie
Embase
|
No. |
Query |
Results |
|
#13 |
#5 AND #10 |
1300 |
|
#12 |
#5 AND #7 |
111 |
|
#11 |
#5 AND #6 |
138 |
|
#10 |
#8 OR #9 |
15670720 |
|
#9 |
'case control study'/de OR 'comparative study'/exp OR 'control group'/de OR 'controlled study'/de OR 'controlled clinical trial'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'phase 2 clinical trial'/de OR 'phase 3 clinical trial'/de OR 'phase 4 clinical trial'/de OR 'pretest posttest design'/de OR 'pretest posttest control group design'/de OR 'quasi experimental study'/de OR 'single blind procedure'/de OR 'triple blind procedure'/de OR (((control OR controlled) NEAR/6 trial):ti,ab,kw) OR (((control OR controlled) NEAR/6 (study OR studies)):ti,ab,kw) OR (((control OR controlled) NEAR/1 active):ti,ab,kw) OR 'open label*':ti,ab,kw OR (((double OR two OR three OR multi OR trial) NEAR/1 (arm OR arms)):ti,ab,kw) OR ((allocat* NEAR/10 (arm OR arms)):ti,ab,kw) OR placebo*:ti,ab,kw OR 'sham-control*':ti,ab,kw OR (((single OR double OR triple OR assessor) NEAR/1 (blind* OR masked)):ti,ab,kw) OR nonrandom*:ti,ab,kw OR 'non-random*':ti,ab,kw OR 'quasi-experiment*':ti,ab,kw OR crossover:ti,ab,kw OR 'cross over':ti,ab,kw OR 'parallel group*':ti,ab,kw OR 'factorial trial':ti,ab,kw OR ((phase NEAR/5 (study OR trial)):ti,ab,kw) OR ((case* NEAR/6 (matched OR control*)):ti,ab,kw) OR ((match* NEAR/6 (pair OR pairs OR cohort* OR control* OR group* OR healthy OR age OR sex OR gender OR patient* OR subject* OR participant*)):ti,ab,kw) OR ((propensity NEAR/6 (scor* OR match*)):ti,ab,kw) OR versus:ti OR vs:ti OR compar*:ti OR ((compar* NEAR/1 study):ti,ab,kw) OR (('major clinical study'/de OR 'clinical study'/de OR 'cohort analysis'/de OR 'observational study'/de OR 'cross-sectional study'/de OR 'multicenter study'/de OR 'correlational study'/de OR 'follow up'/de OR cohort*:ti,ab,kw OR 'follow up':ti,ab,kw OR followup:ti,ab,kw OR longitudinal*:ti,ab,kw OR prospective*:ti,ab,kw OR retrospective*:ti,ab,kw OR observational*:ti,ab,kw OR 'cross sectional*':ti,ab,kw OR cross?ectional*:ti,ab,kw OR multicent*:ti,ab,kw OR 'multi-cent*':ti,ab,kw OR consecutive*:ti,ab,kw) AND (group:ti,ab,kw OR groups:ti,ab,kw OR subgroup*:ti,ab,kw OR versus:ti,ab,kw OR vs:ti,ab,kw OR compar*:ti,ab,kw OR 'odds ratio*':ab OR 'relative odds':ab OR 'risk ratio*':ab OR 'relative risk*':ab OR 'rate ratio':ab OR aor:ab OR arr:ab OR rrr:ab OR ((('or' OR 'rr') NEAR/6 ci):ab))) |
13869826 |
|
#8 |
'major clinical study'/de OR 'clinical study'/de OR 'case control study'/de OR 'family study'/de OR 'longitudinal study'/de OR 'retrospective study'/de OR 'prospective study'/de OR 'comparative study'/de OR 'cohort analysis'/de OR ((cohort NEAR/1 (study OR studies)):ab,ti) OR (('case control' NEAR/1 (study OR studies)):ab,ti) OR (('follow up' NEAR/1 (study OR studies)):ab,ti) OR (observational NEAR/1 (study OR studies)) OR ((epidemiologic NEAR/1 (study OR studies)):ab,ti) OR (('cross sectional' NEAR/1 (study OR studies)):ab,ti) |
7510187 |
|
#7 |
'randomized controlled trial'/exp OR 'randomized controlled trial' OR random*:ti,ab OR (((pragmatic OR practical) NEAR/1 'clinical trial*'):ti,ab) OR ((('non inferiority' OR noninferiority OR superiority OR equivalence) NEAR/3 trial*):ti,ab) OR rct:ti,ab,kw |
2128986 |
|
#6 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
903921 |
|
#5 |
#4 NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
2388 |
|
#4 |
#1 AND #2 AND #3 |
3099 |
|
#3 |
'laparotomy'/exp OR 'celiotom*':ti,ab,kw OR 'laparotom*':ti,ab,kw |
124410 |
|
#2 |
'laparoscopy'/exp OR laparoscop*:ti,ab,kw |
285100 |
|
#1 |
'abdominal injury'/exp OR (((abdomen* OR abdominal) NEAR/4 (injur* OR trauma* OR wound* OR contusion)):ti,ab,kw) OR ((('digestive system' OR perineum OR spleen OR colon) NEAR/3 (injur* OR rupture*)):ti,ab,kw) OR 'vulnus abdominalis':ti,ab,kw OR (((esophagus OR gallbladder OR intestine OR duodenum OR stomach OR ulcer OR liver) NEAR/4 (perforation* OR rupture*)):ti,ab,kw) |
215600 |
Ovid/Medline
|
# |
Searches |
Results |
|
11 |
5 and 8 |
357 |
|
10 |
5 and 7 |
60 |
|
9 |
5 and 6 |
46 |
|
8 |
Epidemiologic studies/ or case control studies/ or exp cohort studies/ or Controlled Before-After Studies/ or Case control.tw. or cohort*.tw. or Cohort analy$.tw. or (Follow up adj (study or studies)).tw. or (observational adj (study or studies)).tw. or Longitudinal.tw. or Retrospective*.tw. or prospective*.tw. or consecutive*.tw. or Cross sectional.tw. or Cross-sectional studies/ or historically controlled study/ or interrupted time series analysis/ |
4413265 |
|
7 |
exp clinical trial/ or randomized controlled trial/ or exp clinical trials as topic/ or randomized controlled trials as topic/ or Random Allocation/ or Double-Blind Method/ or Single-Blind Method/ or (clinical trial, phase i or clinical trial, phase ii or clinical trial, phase iii or clinical trial, phase iv or controlled clinical trial or randomized controlled trial or multicenter study or clinical trial).pt. or random*.ti,ab. or (clinic* adj trial*).tw. or ((singl* or doubl* or treb* or tripl*) adj (blind$3 or mask$3)).tw. or Placebos/ or placebo*.tw. |
2557621 |
|
6 |
(meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf.) not (comment/ or editorial/ or letter/ or ((exp animals/ or exp models, animal/) not humans/)) |
621541 |
|
5 |
4 not ((exp animals/ or exp models, animal/) not humans/) not (letter/ or comment/ or editorial/) |
754 |
|
4 |
1 and 2 and 3 |
790 |
|
3 |
exp Laparotomy/ or celiotom*.ti,ab,kf. or laparotom*.ti,ab,kf. |
65488 |
|
2 |
exp laparoscopy/ or laparoscop*.ti,ab,kf. |
168078 |
|
1 |
exp Abdominal Injuries/ or ((abdomen* or abdominal) adj4 (injur* or trauma* or wound* or contusion)).ti,ab,kf. or (('digestive system' or perineum or spleen or colon) adj3 (injur* or rupture*)).ti,ab,kf. or 'vulnus abdominalis'.ti,ab,kf. or ((esophagus or gallbladder or intestine or duodenum or stomach or ulcer or liver) adj4 (perforation* or rupture*)).ti,ab,kf. |
43292 |