Operatieve behandeling
Uitgangsvraag
Wat is de waarde van een operatieve behandeling na een primaire, anterieure schouderluxatie bij volwassenen?
Aanbeveling
Overweeg in samenspraak met de patiënt een operatieve interventie in geval er sprake is van ten minste één van de onderstaande factoren:
- Leeftijd jonger dan 40 jaar
- Contactsporter
- Significant botverlies
Overweeg in alle overige gevallen een niet-operatieve behandeling van een primaire schouderluxatie bij volwassen patiënten, met name bij patiënten met een tuberculum majus fractuur (zie module prognostische factoren).
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
Er is literatuuronderzoek uitgevoerd naar het effect van operatieve behandeling in vergelijking met niet-operatieve behandeling van een primaire, anterieure schouderluxatie. Recidief van een schouderluxatie en complicaties werden als cruciale uitkomst gedefinieerd. Patiënt-gerapporteerde uitkomsten, gericht op de functie van de schouder en schouder gerelateerde kwaliteit van leven, terugkeer naar sport en/of werk, schouderinstabiliteit, noodzaak tot een operatie en functionele uitkomsten, zoals bewegingsuitslagen en spierkracht werden als belangrijke uitkomsten beschouwd.
Er is redelijk robuuste bewijskracht voor de cruciale uitkomst recidief van een schouderluxatie dat operatieve behandeling van een primaire, anterieure schouderluxatie het risico op recidief aanzienlijk verlaagt vergeleken met een niet-operatieve behandeling bij patiënten met een gemiddelde leeftijd, variërend tussen de studies, van 22-27 jaar. Operatieve behandeling lijkt ook te resulteren in een lager aantal secundaire operaties in vergelijking met niet-operatieve behandeling. De bewijskracht hiervoor is echter laag. De literatuur is onzeker over het effect van operatieve behandeling van een primaire, anterieure schouderluxatie voor de cruciale uitkomst complicaties bij operatieve behandeling en voor de belangrijke uitkomsten patiënt-gerapporteerde uitkomsten, gericht op de functie van de schouder en kwaliteit van leven, terugkeer naar sport, subjectieve schouderinstabiliteit en range of motion van de schouder ten opzichte van niet-operatieve behandeling. Een reden voor de zeer lage bewijskracht is het kleine aantal studies en het kleine aantal patiënten waarop deze uitkomsten werden gebaseerd. De uitkomsten terugkeer naar werk en spierkracht werden op voorhand door de werkgroep als relevante uitkomsten voor deze module gedefinieerd, maar werden in geen van de geïncludeerde studies gerapporteerd. Terugkeer naar sport werd wel gerapporteerd in twee geïncludeerde trials. Hieruit bleek dat, weliswaar met een lage bewijskracht, operatieve behandeling kan resulteren in een grotere kans op terugkeer naar sport dan een conservatieve behandeling van een acute, primaire schouderluxatie.
De studies, die werden gevonden, beschrijven voornamelijk jonge patiënten in de leeftijdsrange van 22-27 jaar. De systematische review van Spanning (2021) beschrijft geen beperking in de leeftijd bij de inclusiecriteria. De studie van Minkus (2021) hanteert een inclusiecriterium van 18-40 en de studie van Pougès (2021) een criterium van 18-25 jaar. Er lijken op voorhand dus al aanwijzingen te zijn bij welke patiënten operatieve behandeling een meerwaarde kan hebben. Op de uitkomstmaat recidief, en in zeker zin ook voor noodzaak tot re-operatie, blijkt operatieve behandeling ook een meerwaarde bij deze groep patiënten te hebben. Voor oudere leeftijdsgroepen is dit niet uit de literatuur te extraheren. Op basis van module 2 lijkt de kans op persisterende danwel recidief instabiliteit na een primaire schouderluxatie af te nemen bij toenemende leeftijd, met name tot 40 jaar. Aangezien het niet aannemelijk is dat fysiologische danwel anatomische factoren verbeteren met de leeftijd lijkt het dat het activiteitenpatroon hierin de belangrijkste overweging is. Op basis van de mogelijke associatie voor recidief danwel persisterende instabiliteitsklachten kan vooral een operatie worden overwogen bij volwassen patiënten (met een leeftijd jonger dan 40 jaar) die aan contactsport doen en met vastgesteld botverlies op de beeldvorming. De kans op een hernieuwd trauma met recidief luxatie als gevolg is naar redenatie groter in deze patiëntencategorie. Een veel gebruikt instrument in de literatuur om tot een keuze voor de juiste operatietechniek te komen bij patiënten met recidiverende instabiliteit is de Instability Severity Index Score (Balg, 2007). In deze score lijst worden zowel deelname aan een contactsport als botverlies aan glenoïd en humerale zijde als een risico factor gezien voor de kans op recidief instabiliteit na een arthroscopische stabilisatie van de schouder middels het hechten van het labrum en verrichten van een capsulair shift (Bankart repair). Zeker in geval van botverlies wordt regelmatig gekozen voor een operatieve behandeling, waarbij er een botblokje aan de voorzijde van het glenoïd wordt geplaatst om hiervoor te corrigeren en de kans op recidief te verkleinen (bijvoorbeeld stabilisatie volgens Latarjet). Deze factoren lijken ook van toepassing op de sportieve, jonge patiënt na een eerste traumatische luxatie die aan een contactsport doet, simpelweg omdat de contactsport het risico op een trauma van de schouder met mogelijke luxatie als gevolg verhoogt.
De kans op recidief of persistente klachten is mogelijk kleiner wanneer er ook sprake is van een tuberculum majus fractuur (zie module prognostisch factoren).
Daarnaast was er sprake van een grote mate van diversiteit in de geïncludeerde studies met betrekking tot de toegepaste chirurgische- en conservatieve interventies. Drie studies voerden een arthroscopische Bankart repair uit (Bottoni, 2002; Pougès, 2021; Yapp, 2020), één studie een open Bankart repair (Jakobsen, 2007), Kirkley (2005) paste een chirurgisch anterieure stabilisatie toe en Minkus (2021) voerde een arthroscopische anterieure stabilisatie van de schouder uit. De conservatieve behandelingen bestonden uit het gebruik van een mitella met een gefaseerde opbouw naar passieve mobilisatie, actieve mobilisatie en krachttraining tot volledig gebruik van de schouder. Echter, de duur van de revalidatieperiode varieerde van vier tot zes maanden. In de studie van Yapp (2020) werd geen verdere informatie beschreven over de inhoud en duur van de conservatieve behandeling. De inhoud van enkele van deze conservatieve behandelingen, zoals gebruik van een mitella met opbouw naar passieve mobilisatie is over het algemeen niet wat de werkgroep zou adviseren (zie module immobilisatie en de module fysiotherapeutische behandeling), waardoor er mogelijk een groter contrast in effect van chirurgische interventie wordt aangetoond in de literatuur. De aanwezige verschillen in chirurgische- en conservatieve behandelingen tussen de studies kunnen invloed hebben, bijvoorbeeld op het aantal terugkerende schouderluxaties, omdat niet duidelijk is welke vorm van chirurgie en welke conservatieve behandeling het meest effectief is om de kans op een herhaalde schouderluxatie te verkleinen. Het verschil in persisterende danwel recidief instabiliteit tussen de operatief behandelde patiënten en de niet operatief behandelde patiënten zal in de praktijk wellicht kleiner zijn. De operaties die beschreven zijn komen overeen met de ingrepen die in de Nederlandse klinische praktijk worden uitgevoerd. De niet-operatieve behandelingen bestaan uit nauwelijks tot geen behandeling tot meer uitgebreide fysiotherapeutische behandeling, waarbij veel patiënten niet behandeld worden volgens de inzichten beschreven in de huidige richtlijn (zie module fysiotherapeutische behandeling).
Waarden en voorkeuren van patiënten (en evt. hun verzorgers)
De operatieve interventie resulteert in minder recidief luxaties maar heeft daarentegen geen bewezen invloed op de PROMS en op de andere uitkomstmaten. Iedere patiënt opereren na een eerste luxatie zou resulteren in overbehandeling. “Shared decision making” met de patiënt is hier aangewezen om de lagere kans op recidief af te wegen tegen het ondergaan van een operatie die niet altijd nodig is om recidief te voorkomen. Nadelen van deze operatie zijn de geassocieerde risico’s, al is het op basis van de analyse van de literatuur in deze richtlijn, vanwege de zeer lage bewijskracht, onduidelijk of complicaties klinisch relevant verschillend zijn ten opzichte van een niet-operatieve behandeling. Voor een hogere kans op recidief na een niet operatief behandelde eerste schouderluxatie verwijst de werkgroep naar module 2 van deze richtlijn. Bij een hogere kans op recidief kan een operatie meer aangewezen zijn. Sommige voorspellers voor recidief na niet-operatieve behandeling van een eerste luxatie zijn de voorspellers van recidief na een operatief (arthroscopische Bankart repair) behandelde patiënt.
Kosten (middelenbeslag)
Operatieve interventies resulteren in minder recidief luxaties bij patiënten in de leeftijdsrange van 22-27 jaar. Deze recidieven, net zoals de operatieve behandeling, gaan aannemelijk gepaard met directe en indirecte zorgkosten. Een operatie voorkomt vaker een tweede en volgende luxatie en zou hierdoor kosteneffectief kunnen zijn. Hier geldt dat niet iedere uitgevoerde operatie voor een eerste luxatie daadwerkelijk een recidief voorkomt. Er is beperkt bewijs dat chirurgie meer kosteneffectief is dan een niet-operatieve behandeling (Crall, 2012).
Aanvaardbaarheid, haalbaarheid en implementatie
De operatieve en niet operatieve interventies zoals beschreven in de studies en in deze paragraaf worden sinds lange tijd toegepast. De afgelopen jaren is veel aanvullend inzicht verkregen in de voorspellers voor uitkomst na behandeling van anterieure instabiliteit. De trend naar het vaker kiezen voor een operatieve interventie na een eerste anterieure schouderluxatie bij een subgroep patiënten wordt ondersteund door deze richtlijn.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Uit de literatuur blijkt dat een operatieve behandeling bij patiënten met een leeftijd jonger dan 40 jaar leidt tot minder recidief. De operatieve interventie resulteert bij patiënten onder de 40 jaar in minder recidief luxaties, maar heeft daarentegen geen bewezen invloed op de PROMS en op de andere uitkomstmaten. Iedere patiënt opereren na een eerste luxatie zou resulteren in overbehandeling. Bij een hogere kans op recidief vanwege de aanwezigheid van verscheidene prognostische factoren die de kans op recidief danwel persisterende klachten vergroten kan, in overleg met de patiënt, een operatie meer aangewezen zijn. Hiervoor zijn voorzichtige aanwijzingen vanuit module 2, welke worden ondersteund door expert opinion. Een operatieve ingreep kan vooral worden overwogen bij patiënten met een leeftijd jonger dan 40 jaar, iemand die aan contactsport doet en/of significant botverlies vertoont op beeldvorming. Gezien het feit dat persisterende klachten minder voorkomen na een tuberculum majus fractuur is een operatieve ingreep in dit geval niet de eerste keuze van behandeling.
Onderbouwing
Er is een voortdurende discussie over het al dan niet operatief behandelen van een eerste anterieure schouderluxatie. Het hoge percentage complicaties, vooral bij jonge volwassenen, zoals terugkerende instabiliteit, restklachten en onvermogen om weer te gaan sporten na niet-operatieve behandeling, kan erop wijzen dat operatieve behandeling een meerwaarde heeft.
1. Recurrence (critical)
|
Moderate GRADE |
Operative treatment likely reduces recurrence of shoulder dislocations when compared with non-operative treatment in adult patients (with mean ages ranging between studies from 22 to 27 years) with a primary, anterior shoulder dislocation.
Sources: van Spanning (2021) (Bottoni, 2002; Jakobsen, 2007; Kirkley, 2005; Yapp, 2020); Minkus (2021); Pougès (2021). |
2. Complications (critical)
|
Very low GRADE |
The evidence is very uncertain whether operative treatment for primary anterior shoulder dislocations reduces complications (other than recurrence) when compared with non-operative treatment in adult patients (with a mean age of mean age of around 22 to 27 years) with a primary, anterior shoulder dislocation.
Sources: Minkus (2021). |
3. Patient reported outcomes (important)
|
Very low GRADE |
3.1 WOSI The evidence is very uncertain whether operative treatment for primary anterior shoulder dislocations improves shoulder related quality of life when compared with non-operative treatment in adult patients (with mean ages ranging between studies from 22 to 27 years) with a primary, anterior shoulder dislocation.
Sources: Pougès (2021).
3.2 Rowe; 3.3 Constant-Murley Shoulder Outcome Score; 3.4 Subjective Shoulder Value The evidence is very uncertain whether operative treatment improves shoulder function when compared with non-operative treatment in patients with primary, anterior shoulder dislocations in adult patients (with a mean age of mean age of around 22 to 27 years) with a primary, anterior shoulder dislocation.
Sources: Minkus (2021). |
4. Need for (secondary) surgery (important)
|
Low GRADE |
Operative treatment may reduce the need for (secondary) surgery when compared with non-operative treatment in adult patients (with a mean age of mean age of around 22 to 27 years). with a primary, anterior shoulder dislocation.
Sources: van Spanning (2021) (Bottoni, 2002; Jakobsen, 2007); Minkus (2021); Pougès (2021). |
5. Return to sport (important)
|
Low GRADE |
Operative treatment may result in more patients who return to sport when compared with non-operative treatment in adult patients (with mean ages ranging between studies from 22 to 27 years) with a primary, anterior shoulder dislocation.
Sources: Pougès (2021); Yapp (2020). |
6. Return to work (important)
|
No GRADE |
No evidence was found regarding the effect of operative treatment on return to work when compared with non-operative treatment in adult patients with a primary, anterior shoulder dislocation.
Sources: - |
7. Shoulder instability (important) (Instability symptoms among patients who did not have a recurrent instability event and measured instability with the apprehension test)
|
Very low GRADE |
The evidence is very uncertain whether operative treatment for primary anterior shoulder dislocations reduces shoulder instability when compared with non-operative treatment in adult patients (with mean ages ranging between studies from 22 to 27 years) with a primary, anterior shoulder dislocation.
Sources: Minkus (2021). |
8. Functional outcomes (important)
|
Very low GRADE |
8.1 Range of motion The evidence is very uncertain whether operative treatment for primary anterior shoulder dislocations improves range of motion when compared with non-operative treatment in adult patients (with mean ages ranging between studies from 22 to 27 years) with a primary, anterior shoulder dislocation.
Sources: Minkus (2021); Pougès (2021). |
|
No GRADE |
8.2 Muscle strength No evidence was found regarding the effect of operative treatment on muscle strength when compared with non-operative treatment in adult patients with a primary, anterior shoulder dislocation.
Sources: - |
Description of studies
Systematic review
The systematic review of Van Spanning (2021) compared operative treatment versus non-operative treatment (NTFD) in patients with first-time anterior shoulder dislocation (OTFD). Van Spanning (2021) searched the electronic databases of Pubmed (Legacy), Embase/Ovid, Cochrane Database of Systematic Reviews/Wiley, Cochrane Central Register of Controlled Trials/Wiley, and Web of Science/Clarivate Analytics from 1990 up to the 15th of April 2020. No language restrictions were applied to the search. Randomized controlled trials and cohort studies with a prospective design comparing recurrence following OTFD and NTFD with a minimum mean follow-up of two years were included. Studies that did not report original data, abstracts, and animal, cadaveric, and biomechanical studies were excluded. Studies reporting outcomes or revision surgery after any previous anterior shoulder stabilization procedure and studies in which patients received arthroplasty were excluded as well. In total, four RCTs, with a total of 192 patients, were included (Bottoni, 2002; Jakobsen, 2007; Kirkley, 2005; Yapp, 2020). The other eight studies were excluded for this guideline. This guideline only includes RCTs and these studies had a prospective, or retrospective observational design or did not compare operative treatment with non-operative treatment. Bottoni (2002) compared arthroscopic Bankart repair with four weeks sling immobilization and limited active motion in patients with primary shoulder dislocations who were in military service. The first phase consisted of sling immobilization for four weeks with limited active range of motion (Codman’s exercises and isometric muscle contractions). The second phase, lasting four weeks, consisted of progressive passive motion exercises without resistance. The third four-week phase focused on restoration of full active range of motion with progressively greater resistance exercises. Return to full active duty, contact sports, and activities requiring overhead or heavy lifting were restricted until four months postoperatively. The primary outcome was either a second dislocation, symptomatic subluxation, or instability preventing return to full active duty or necessitating an additional surgical stabilization. Both groups underwent the same therapist-supervised three-phase rehabilitation program. Jakobsen (2007) compared open Bankart repair with non-operative treatment. Patients in both groups had a non-fixed sling for one week, after which both groups underwent an identical rehabilitation program consisting of passive movement immediately postoperatively without rotating, lifting, and pushing. At three weeks postoperatively, active internal rotation and abduction were permitted, and after eight weeks, external rotation exercises were introduced. Swimming and light sports were allowed after twelve weeks and overhead sports after six months. Both groups underwent an identical rehabilitation program. Jakobsen (2007) did not describe the criteria for the need for (secondary) surgery. Kirkley (2005) compared immediate anterior stabilization plus rehabilitation with immobilization for three weeks followed by identical rehabilitation, which was started three weeks after the dislocation. The rehabilitation protocol consisted of three stages. In stage one (week four to six) the patients were allowed to perform active-assisted range of motion with external rotation limited to twenty degrees. During stage two (weeks seven to eight), patients were allowed to perform isometric strengthening exercises and external rotation of 45 degrees. In stage three (week nine to twelve) patients started with isotonic strengthening, active range of motion with terminal stretch and limited return to sports at three months. At week sixteen, return to full sporting activities was allowed. Patients in both groups were allowed to undergo further surgical intervention if they declared themselves as having recurrent symptomatic instability episodes at any time during the study. Yapp (2020) compared an arthroscopic Bankart repair with an arthroscopic washout. All patients received standard non-operative rehabilitation for a primary traumatic anterior shoulder dislocation. Rehabilitation was not further described. All patients who experienced recurrent instability underwent radiographic investigation and were offered further surgery based on soft-tissue or osseous pathology, regardless of their initial treatment allocation. The mean age of enrolled patients in the studies was around 22 to 25 years and the overall population consisted of 169 males and 23 females. The length of follow-up between the included studies varied between three and ten years. Risk of bias was assessed with the revised tool developed by Cochrane. The reported outcomes in the study were recurrence rates and need for (secondary) surgery.
Randomized controlled trials
The multicenter randomized controlled trial of Minkus (2021) aimed to compare outcomes of arthroscopic shoulder stabilization with immobilization in non-operative treatment in patients with a primary shoulder dislocation. Non-operative treatment was defined as immobilization with the shoulder in 60 degrees of external rotation and 30 degrees abduction. In total, 112 patients were randomized. Patients in the operative treatment group (n=52; mean age 25.7 (SD 6.2) years) underwent surgery within three weeks after trauma. Postoperatively, the patients were immobilized in internal rotation for three weeks, and a standardized rehabilitation protocol was performed. Patients in the non-operative group (n=60; mean age 26.7 (SD 5.8) years) underwent non-operative treatment beginning at least three days after trauma. Patients were instructed to wear the brace 24 hours a day, for three weeks in total. Free passive and active range of motion exercises were allowed six weeks after first-time shoulder dislocation for the immobilization group and six weeks after operative stabilization. Eight patients in the operative treatment group and nine patients in the non-operative treatment group were lost to follow-up. Length of follow-up assessment was two years. The reported outcomes in the study were overall recurrence of shoulder instability, adverse outcomes, patient reported outcomes, such as the Western Ontario Shoulder Instability Index (WOSI) score, the Rowe-score, the Constant-Murley score, and the Subjective Shoulder Value (SSV), need for (secondary) surgery and functional outcomes, such as shoulder instability and range of motion.
The randomized controlled trial of Pougès (2021) aimed to compare outcomes for operative treatment with arthroscopic Bankart repair versus non-operative treatment in patients with first-time anterior shoulder dislocation. In total, 40 patients were randomized. Patients in the operative treatment group (n=20; median age 22 (IQR 20.5 to 22.5) years) underwent arthroscopic Bankart repair. Surgery was performed in the first fifteen days after the first episode of anterior shoulder dislocation. Internal rotation immobilization was to be followed for the first three weeks after the surgery. Patients in the non-operative treatment group (n=20; median age 21.5 (IQR 20 to 22.5 years) were immobilized for three weeks after anterior shoulder dislocation. Both treatment groups followed the same physical therapy protocol. Physical therapy began at three weeks and consisted of passive and active mobilization while limiting external rotation to 30 degrees and abduction to 90 degrees. Unlimited range of motion was allowed after six weeks. None of the patients were lost to follow-up. Maximum length of follow-up assessment was two years. The reported outcomes in the study were overall recurrence of shoulder instability, patient reported outcomes, such as the WOSI-score, Walch-Duplay score, and the QuickDASH score, need for (secondary) surgery, functional outcomes, such as range of motion, return to sport, and patient satisfaction.
Results
1. Recurrence of shoulder dislocation (critical)
Recurrence of shoulder dislocation at a minimum of two years follow-up was reported in four studies, retrieved from the systematic review of van Spanning (2021) (Bottoni, 2002; Jakobsen, 2007; Kirkley, 2005; Yapp, 2020) and in two additional studies (Minkus, 2021; Pougès, 2021). The results were pooled in a meta-analysis. The pooled number of patients with recurrence of shoulder dislocation in the operative treatment group was 14/157 (8.9%), compared to 80/164 (48.8%) in the non-operative treatment group. This resulted in a pooled relative risk ratio (RR) of 0.20 (95% CI 0.12 to 0.33), in favor of the operative treatment group. This is considered as a clinically relevant difference.
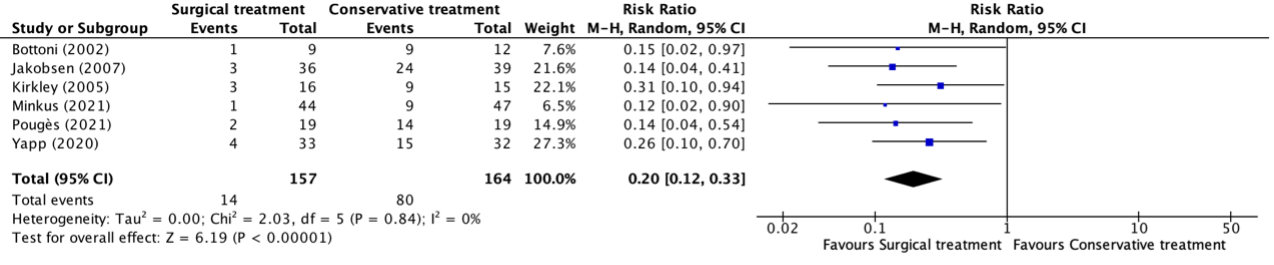
Figure 1. Forest plot showing the comparison between operative treatment and non-operative treatment for recurrence of shoulder dislocation. Pooled relative risk ratio, random effects model. Z: p-value of overall effect; df: degrees of freedom; I2; statistical heterogeneity; CI: confidence interval.
2. Complications (critical)
Complications at a minimum of two years follow-up were reported in one study (Minkus, 2021). Minkus (2021) defined complications as adverse events, apart from recurrent dislocations, that occurred after operative shoulder stabilization or after immobilization treatment. In both groups, the number of patients with complications was 0 (0%). This is not considered as a clinically relevant difference.
3. Patient reported outcomes (important)
Western Ontario Shoulder Instability Index (WOSI)
The WOSI-score at a minimum of two years follow-up was reported in one study (Pougès, 2021).
The mean (SD) WOSI-score in the study of Pougès (2021) in the operative treatment group (n=20) was 11.5 (18.6) points, compared to 17.7 (18.4) in the non-operative treatment group (n=20). This resulted in a mean difference (MD) of -6.20 (95% CI -17.96 to 5.56) points, in favor of the operative treatment group. This is not considered as a clinically relevant difference.
Rowe
The Rowe-score at a minimum of two years follow-up was reported in one study (Minkus, 2021). The mean (SD) Rowe-score in the operative treatment group (n=44) was 88.5 (11.2) points, compared to 89.1 (7.1) points in the non-operative treatment group (n=47). This resulted in a mean difference (MD) of 0.60 (95% CI -3.28 to 4.48) points, in favor of the non-operative treatment group. This is not considered as a clinically relevant difference.
Constant-Murley Shoulder Outcome Score
The Constant-Murley Outcome Score at two years follow-up was reported in one study (Minkus, 2021). The mean (SD) Constant-Murley Outcome Score in the operative treatment group (n=44) was 93.9 (10.1) points, compared to 96.9 (4.7) points in the non-operative treatment group (n=47). This resulted in a mean difference (MD) of 3.00 (95% CI -0.27 to 6.27) points, in favor of the non-operative treatment group. This is not considered as a clinically relevant difference.
Subjective Shoulder Value
The Subjective Shoulder Value score at a minimum of two years follow-up was reported in one study (Minkus, 2021). The mean (SD) Subjective Shoulder Value in the operative treatment group (n=44) was 93.1% (6.5), compared to 93.6% (4.4) in the non-operative treatment group (n=47). This resulted in a mean difference (MD) of 0.50 (95% CI -1.80 to 2.80), in favor of the non-operative treatment group. This is not considered as a clinically relevant difference.
4. Need for (secondary) surgery (important)
Need for (secondary) surgery at a minimum of two years follow-up was reported in three studies, retrieved from the systematic review of van Spanning (2021) (Bottoni, 2002; Jakobsen, 2007; Yapp, 2020) and in two additional studies (Minkus, 2021; Pougès, 2021). The studies had different criteria for the need for (secondary) surgery:
- The criteria used to define the treatment as a failure in the study of Bottoni (2002) was either a second dislocation or symptomatic subluxation or instability preventing return to full active duty or necessitating an additional surgical stabilization.
- All patients in the study of Yapp (2020) who experienced recurrent instability underwent radiographic investigation and were offered further surgery based on soft-tissue or osseous pathology, regardless of their initial treatment allocation.
- The study of Pougès (2021) did not report specific criteria for the need for (secondary) surgery, but reported that patients who experienced multiple subluxations, underwent (secondary) surgery.
- The studies of Jakobsen (2007) and Minkus (2021) did not report criteria for the need for (secondary) surgery.
The results were pooled in a meta-analysis. The pooled number of patients that needed (secondary) surgery in the operative treatment group was 6/141 (4.3%), compared to 43/149 (28.9%) in the non-operative treatment group. This resulted in a pooled relative risk ratio (RR) of 0.20 (95% CI 0.03 to 0.40), in favor of the operative treatment group. This is considered as a clinically relevant difference.

Figure 2. Forest plot showing the comparison between operative treatment and non-operative treatment for need for (secondary) surgery. Pooled relative risk ratio, random effects model. Z: p-value of overall effect; df: degrees of freedom; I2; statistical heterogeneity; CI: confidence interval.
5. Return to sport (important)
Return to sport at a minimum of two years follow-up was reported in one study, retrieved from the systematic review of van Spanning (2021) (Yapp, 2020) and in one additional study (Pougès, 2021). The results were pooled in a meta-analysis. The pooled number of patients who returned to sport in the operative treatment group was 46/51 (90.2%), compared to 32/52 (61.5%) in the non-operative treatment group. This resulted in a pooled relative risk ratio (RR) of 0.69 (95% CI 0.55 to 0.87), in favor of the operative treatment group. This is considered as a clinically relevant difference.

Figure 3. Forest plot showing the comparison between operative treatment and non-operative treatment for return to sport. Pooled relative risk ratio, random effects model. Z: p-value of overall effect; df: degrees of freedom; I2; statistical heterogeneity; CI: confidence interval.
6. Return to work (important)
None of the included studies reported information regarding the outcome return to work for operative treatment of shoulder dislocations versus non-operative treatment in patients with primary, anterior shoulder dislocations.
7. Shoulder instability (important)
Shoulder instability was reported in one study (Minkus, 2021). Minkus (2021) defined shoulder instability as instability symptoms among patients who did not have a recurrent instability event and measured instability with the apprehension test.
The number of patients with a positive apprehension test at two years follow-up in the operative treatment group was 2/44 (4.7%), compared to 3/47 (7.9%) in the non-operative treatment group. This resulted in a relative risk ratio (RR) of 0.71 (95% CI 0.12 to 4.06), in favor of the operative treatment group. This is not considered as a clinically relevant difference.
8. Functional outcomes (important)
Range of motion: external rotation in 90 degrees of abduction
External rotation with the arm in 90 degrees of abduction was reported in two studies (Minkus, 2021; Pougès, 2021). Minkus (2021) reported the total range of motion in external rotation with the arm in 90 degrees abduction. Pougès (2021) reported the range of motion of external rotation in comparison with the uninjured side.
The mean (SD) range of motion of external rotation with the arm in 90 degrees of abduction at two years follow-up in the study of Minkus (2021) in the operative treatment group (n=44) was 80.0 (12.0) degrees, compared to 86.0 (9.0) degrees in the non-operative treatment group (n=47). This resulted in a mean difference (MD) of 6.00 (95% CI 1.62 to 10.38) degrees, in favor of the non-operative treatment group. This is not considered as a clinically relevant difference.
The study of Pougès (2021) reported the mean range of motion of anterior elevation, abduction, extension, external rotation with the arm in zero degrees of abduction, external rotation with the arm in 90 degrees of abduction, and internal rotation at two years follow-up. The results are depicted in table 1:
Table 1: mean differences in range of motion of the injured side in comparison with the uninjured side
|
|
Mean difference (SD) in comparison with the uninjured side for the operative treatment group (n=20) |
Mean difference in comparison with the uninjured side for the non-operative treatment group (n=20) |
|
Anterior elevation |
-0.5 (2.3) degrees |
2.1 (7.1) degrees |
|
Abduction |
0.5 (2.3) degrees |
5.8 (11.7) degrees |
|
Extension |
3.2 (8.2) degrees |
2.1 (7.9) degrees |
|
External rotation (with the arm in zero degrees of abduction) |
-1.5 (6.7) degrees |
3.7 (7.0) degrees |
|
External rotation with the arm in 90 degrees of abduction |
0.5 (5.2) degrees |
3.1 (8.2) degrees |
|
Internal rotation |
19.0 (not reported) degrees |
19.0 (not reported) degrees |
Muscle strength
None of the included studies reported information regarding the outcome muscle strength for operative treatment of shoulder dislocations versus non-operative treatment in patients with primary, anterior shoulder dislocations.
Level of evidence of the literature
1. Recurrence
The level of evidence regarding the outcome measure recurrence was derived from randomized controlled trials and therefore started high. The level of evidence was downgraded by one level because of a lack of blinding of patients and study personnel in the studies (risk of bias, -1). The level of evidence is moderate.
2. Complications
The level of evidence regarding the outcome measure complications was derived from randomized controlled trials and therefore started high. The level of evidence was downgraded by three levels because of a lack of blinding of patients and study personnel in the study (risk of bias, -1) and the small number of events and the small number of events in the study (imprecision, -2). The level of evidence was very low.
3. Patient reported outcomes
3.1 WOSI
The level of evidence regarding the outcome measure WOSI for shoulder related quality of life was derived from randomized controlled trials and therefore started high. The level of evidence was downgraded by three levels because of a lack of blinding of patients and study personnel in the studies (risk of bias, -1), the wide confidence interval crossing the upper border of clinical relevance, and the small number of patients in the studies (imprecision, -2). The level of evidence was very low.
3.2 Rowe
The level of evidence regarding the outcome measure Rowe-score for the function of the shoulder was derived from randomized controlled trials and therefore started high. The level of evidence was downgraded by three levels because of a lack of blinding of patients and study personnel in the studies (risk of bias, -1) and the small number of patients in the studies (imprecision, -2). The level of evidence was very low.
3.3 Constant-Murley Shoulder Outcome Score
The level of evidence regarding the outcome measure Constant-Murley Shoulder Outcome Score for the function of the shoulder was derived from randomized controlled trials and therefore started high. The level of evidence was downgraded by three levels because of a lack of blinding of patients and study personnel in the studies (risk of bias, -1) and the small number of patients in the studies (imprecision, -1). The level of evidence was very low.
3.4 Subjective Shoulder Value
The level of evidence regarding the outcome measure SSV for the function of the shoulder was derived from randomized controlled trials and therefore started high. The level of evidence was downgraded by two levels because of a lack of blinding of patients and study personnel in the studies (risk of bias, -1) and the small number of patients in the studies (imprecision, -1). The level of evidence was low.
4. Need for (secondary) surgery
The level of evidence regarding the outcome measure need for (secondary) surgery was derived from randomized controlled trials and therefore started high. The level of evidence was downgraded by two levels because of a lack of blinding of patients and study personnel in the studies (risk of bias, -1) and the small number of events in the studies (imprecision, -1). The level of evidence is low.
5. Return to sport
The level of evidence regarding the outcome measure return to sport was derived from randomized controlled trials and therefore started high. The level of evidence was downgraded by two levels because of a lack of blinding of patients and study personnel in one of the studies (risk of bias, -1), the wide confidence interval crossing the upper border of clinical relevance, and the small number of patients in the studies (imprecision, -1). The level of evidence is low.
6. Return to work
Because of a lack of data, it was not possible to grade the literature for the outcome return to work in patients with a primary, anterior shoulder dislocation undergoing operative treatment compared with non-operative treatment.
7. Shoulder instability
The level of evidence regarding the outcome measure shoulder instability was derived from randomized controlled trials and therefore started high. The level of evidence was downgraded by three levels because of a lack of blinding of patients and study personnel in the study (risk of bias, -1), the wide confidence interval crossing both borders of clinical relevance, and the small number of events (imprecision, -2). The level of evidence was very low.
8. Functional outcomes
8.1 Range of motion
The level of evidence regarding the outcome measure range of motion was derived from randomized controlled trials and therefore started high. The level of evidence was downgraded by three levels because of a lack of blinding of patients and study personnel in the study (risk of bias, -1), the wide confidence interval crossing the upper border of clinical relevance, and the small number of patients in the studies (imprecision, -2). The level of evidence was very low.
8.2 Muscle strength
Because of a lack of data, it was not possible to grade the literature for the outcome muscle strength in patients with a primary, anterior shoulder dislocation undergoing operative treatment compared with non-operative treatment.
A systematic review of the literature was performed to answer the following question: What is the value of operative treatment for a primary anterior shoulder dislocation in adults?
P: Adult patients with a primary, anterior shoulder dislocation.
I: Operative treatment.
C: Non-operative treatment.
O: Recurrence of shoulder dislocation (symptomatic subluxation or instability); complications; validated patient reported outcome measures (such as Western Ontario Shoulder Instability Index (WOSI), Oxford Shoulder Instability Score (OSIS), Rowe score for instability, Constant-Murley Shoulder Outcome Score, Subjective Shoulder Value; need for (secondary) surgery; return to sport; return to work; shoulder instability (measured with the apprehension test), and functional outcomes (muscle strength, range of motion).
Relevant outcome measures
The working group considered the following outcome parameters to be critical for clinical decision making: recurrence of shoulder dislocation (symptomatic subluxation or instability) and complications. Patient reported outcome measures (such as Western Ontario Shoulder Instability Index (WOSI)*, Oxford Shoulder Instability Score (OSIS), Rowe score for instability**, Constant-Murley Shoulder Outcome Score***, Subjective Shoulder Value (SSV)****; return to sport; return to work; shoulder instability (measured with the apprehension test); need for (secondary) surgery; and functional outcomes (muscle strength and range of motion) were considered as important outcome measures for decision making.
*The WOSI is a 21-item scale used to measure shoulder related quality of life in patients with symptomatic shoulder instability. Each item falls into one of the four domains: (I) physical symptoms; (II) sports, recreation, and work; (III) lifestyle; and (IV) emotion. A score of zero indicates the best possible score, which means that the patient does not experience a decrease in shoulder related quality of life, whereas a score of 100 indicates the highest decrease in shoulder related quality of life.
**The Rowe score is a scoring system for the functional assessment of the shoulder by measuring three domains: (I) stability; (II) motion; and (III) function of the shoulder. The score ranges from zero to 100, in which a score of zero indicates poor or less shoulder function and a score of 100 indicates excellent shoulder function.
***The Constant-Murley Shoulder Outcome Score is a combined scoring system to evaluate the functional status of the shoulder in patients with shoulder pain on a scale from zero to 100. The first part of the questionnaire is completed by the patient, whereas the second part of the questionnaire is completed by the examiner. A score of 100 on the Constant-Murley Outcome Score correspondents with a well-functioning shoulder.
****The Subjective Shoulder Value is a self-reported questionnaire that measures the function of the injured shoulder as estimated in percentages by the patient in comparison with a normally functioning shoulder.
The working group defined a threshold of 10% for continuous outcomes and a relative risk (RR) for dichotomous outcomes of <0.80 and >1.25 between the two treatments as a minimal clinically important difference.
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms until the 10th of February 2022. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 165 hits. First, systematic reviews were selected comparing operative treatment with non-operative treatment for shoulder dislocations. Eleven systematic reviews were initially selected based on title and abstract screening. After reading the full-text, ten systematic reviews were excluded (see table with reasons for exclusion under the tab Methods), and one systematic review was included. The search strategy of this systematic review was completed up to the 15th of April 2020.
Secondly, two randomized controlled trials (RCTs) were selected which were published from the 15th of April 2020 until the 17th of March 2022. These two RCTs were initially selected based on title and abstract screening. After reading the full text, both studies were included.
Results
Three studies were included in the analysis of the literature. Important study characteristics and results are summarized in the evidence tables. The assessment of the risk of bias is summarized in the risk of bias tables.
- Balg F, Boileau P. The instability severity index score. A simple pre-operative score to select patients for arthroscopic or open shoulder stabilisation. J Bone Joint Surg Br. 2007 Nov;89(11):1470-7. doi: 10.1302/0301-620X.89B11.18962. PMID: 17998184.Bottoni CR, Wilckens JH, DeBerardino TM, D'Alleyrand JC, Rooney RC, Harpstrite JK, Arciero RA. A prospective, randomized evaluation of arthroscopic stabilization versus nonoperative treatment in patients with acute, traumatic, first-time shoulder dislocations. Am J Sports Med. 2002 Jul-Aug;30(4):576-80. doi: 10.1177/03635465020300041801. PMID: 12130413.
- Crall TS, Bishop JA, Guttman D, Kocher M, Bozic K, Lubowitz JH. Cost-effectiveness analysis of primary arthroscopic stabilization versus nonoperative treatment for first-time anterior glenohumeral dislocations. Arthroscopy. 2012 Dec;28(12):1755-65. doi: 10.1016/j.arthro.2012.05.885. Epub 2012 Oct 5. PMID: 23040837.
- Jakobsen BW, Johannsen HV, Suder P, Søjbjerg JO. Primary repair versus conservative treatment of first-time traumatic anterior dislocation of the shoulder: a randomized study with 10-year follow-up. Arthroscopy. 2007 Feb;23(2):118-23. doi: 10.1016/j.arthro.2006.11.004. PMID: 17276217.
- Kirkley A, Werstine R, Ratjek A, Griffin S. Prospective randomized clinical trial comparing the effectiveness of immediate arthroscopic stabilization versus immobilization and rehabilitation in first traumatic anterior dislocations of the shoulder: long-term evaluation. Arthroscopy. 2005 Jan;21(1):55-63. doi: 10.1016/j.arthro.2004.09.018. PMID: 15650667.
- Marigi EM, Wilbur RR, Song BM, Krych AJ, Okoroha KR, Camp CL. The Nonoperative Instability Severity Index Score: Is It Predictive in a Larger Shoulder Instability Population at Long-Term Follow-Up? Arthroscopy. 2022 Jan;38(1):22-27. doi: 10.1016/j.arthro.2021.05.021. Epub 2021 May 27. PMID: 34052376.
- Minkus M, Königshausen M, Maier D, Mauch F, Stein T, Greiner S, Moursy M, Scheibel M. Immobilization in External Rotation and Abduction Versus Arthroscopic Stabilization After First-Time Anterior Shoulder Dislocation: A Multicenter Randomized Controlled Trial. Am J Sports Med. 2021 Mar;49(4):857-865. doi: 10.1177/0363546520987823. Epub 2021 Feb 17. PMID: 33596092; PMCID: PMC7961655.
- Olds M, Ellis R, Donaldson K, Parmar P, Kersten P. Risk factors which predispose first-time traumatic anterior shoulder dislocations to recurrent instability in adults: a systematic review and meta-analysis. Br J Sports Med. 2015 Jul;49(14):913-22. doi: 10.1136/bjsports-2014-094342. Epub 2015 Apr 21. PMID: 25900943; PMCID: PMC4687692.
- Pougès C, Hardy A, Vervoort T, Amouyel T, Duriez P, Lalanne C, Szymanski C, Deken V, Chantelot C, Upex P, Maynou C. Arthroscopic Bankart Repair Versus Immobilization for First Episode of Anterior Shoulder Dislocation Before the Age of 25: A Randomized Controlled Trial. Am J Sports Med. 2021 Apr;49(5):1166-1174. doi: 10.1177/0363546521996381. Epub 2021 Mar 11. PMID: 33705240.
- Randelli P, Ragone V, Carminati S, Cabitza P. Risk factors for recurrence after Bankart repair a systematic review. Knee Surg Sports Traumatol Arthrosc. 2012 Nov;20(11):2129-38. doi: 10.1007/s00167-012-2140-1. Epub 2012 Jul 27. PMID: 22836228.
- Tokish JM, Thigpen CA, Kissenberth MJ, Tolan SJ, Lonergan KT, Tokish JM Jr, Dickens JF, Hawkins RJ, Shanley E. The Nonoperative Instability Severity Index Score (NISIS): A Simple Tool to Guide Operative Versus Nonoperative Treatment of the Unstable Shoulder. Sports Health. 2020 Nov/Dec;12(6):598-602. doi: 10.1177/1941738120925738. Epub 2020 Jul 1. PMID: 32609577; PMCID: PMC7785891.
- van Spanning SH, Verweij LPE, Priester-Vink S, van Deurzen DFP, van den Bekerom MPJ. Operative Versus Nonoperative Treatment Following First-Time Anterior Shoulder Dislocation: A Systematic Review and Meta-Analysis. JBJS Rev. 2021 Sep 23;9(9). doi: 10.2106/JBJS.RVW.20.00232. PMID: 35102053.
- Verweij LPE, van Spanning SH, Grillo A, Kerkhoffs GMMJ, Priester-Vink S, van Deurzen DFP, van den Bekerom MPJ. Age, participation in competitive sports, bony lesions, ALPSA lesions, > 1 preoperative dislocations, surgical delay and ISIS score > 3 are risk factors for recurrence following arthroscopic Bankart repair: a systematic review and meta-analysis of 4584 shoulders. Knee Surg Sports Traumatol Arthrosc. 2021 Dec;29(12):4004-4014. doi: 10.1007/s00167-021-06704-7. Epub 2021 Aug 22. PMID: 34420117; PMCID: PMC8595227.
- Waterman BR, Bullock G. Editorial Commentary: The Nonoperative Instability Severity Index Score Can, in Part, Help to Predict Failure After Nonoperative Management of Anterior Shoulder Instability: Fix Them All Versus Wait and See? Arthroscopy. 2022 Jan;38(1):28-30. doi: 10.1016/j.arthro.2021.07.034. PMID: 34972556.
- Yapp LZ, Nicholson JA, Robinson CM. Primary Arthroscopic Stabilization for a First-Time Anterior Dislocation of the Shoulder: Long-Term Follow-up of a Randomized, Double-Blinded Trial. J Bone Joint Surg Am. 2020 Mar 18;102(6):460-467. doi: 10.2106/JBJS.19.00858. PMID: 31895236.
Evidence tabel
Systematic review(s)
|
Study reference |
Study characteristics |
Patient characteristics |
Intervention (I) |
Comparison / control (C)
|
Follow-up |
Outcome measures and effect size |
|
van Spanning (2021) |
SR and meta-analysis of RCTs and prospective or retrospective cohort studies.
For the purpose of this guideline, only the RCTs of the SR of van Spanning were included.
Literature search from 1990 up to April 15, 2020.
Study design: RCT parallel
Setting and Country:
Source of funding There was no funding for this project.
Conflicts of interest: |
Inclusion criteria SR:
Exclusion criteria SR:
15 studies included. For the purpose of this guideline, 11 studies were excluded and 4 studies were included.
Important patient characteristics at baseline:
N (intervention vs control)
mean age (intervention vs control)
Sex:
Mean follow-up (intervention vs control)
Groups comparable at baseline? Yes. |
Describe intervention:
|
Describe control:
|
End-point of follow-up (intervention vs control):
|
Outcome measure 1: Recurrence
A (Bottoni, 2002) I: 1/9 (11.1%) C: 9/12 (75%) RR 0.15 (95% CI 0.02 to 0.97)
B (Jakobsen, 2007) I: 3/36 (8.3%) C: 24/39 (61.5%) RR 0.14 (95% CI 0.04 to 0.41)
C (Kirkley, 2005) I: 3/16 (18.98%) C: 9/15 (60%) RR 0.31 (95% CI 0.10 to 0.94)
D (Yapp, 2020) I: 4/33 C: 15/32 RR 0.26 (95% CI 0.10 to 0.70)
Outcome measure 2: Return to sport D (Yapp, 2020) I: 28/32 (87.5%) C: 19/33 (57.6%)
Outcome measure 3: Return to sport at pre-injury level
D (Yapp, 2020) I: 28/32 (87.5%) C: 19/33 (57.6%)
Outcome measure 4: Need for (secondary) surgery
A (Bottoni, 2002) I: 1/9 (11.1%) C: 6/12 (50%) RR 0.22 (95% CI 0.03 to 1.53)
B (Jakobsen, 2007) I: 1/36 (2.8%) C: 19/39 (48.7%)
|
Randomized controlled trial(s)
|
Study reference |
Study characteristics |
Patient characteristics 2 |
Intervention (I) |
Comparison / control (C) 3
|
Follow-up |
Outcome measures and effect size 4 |
Comments |
|
Minkus (2021) |
Type of study: Multicenter prospective randomized controlled trial.
Setting and country: Seven departments specializing in shoulder and elbow surgery throughout Germany.
Funding: Financial support was provided by the Wilhelm Julius Teufel Company, which assisted this study. M.S., D.M., F.M., T.S., and S.G. received consultant payments from Arthrex that were not related to this work.
Conflicts of interest: AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
|
Inclusion criteria:
Exclusion criteria:
N total at baseline: Intervention: N=52 Control: N=60
Important prognostic factors2: Age, mean (SD) / median (IQR) I: 25.7 (6.2) years C: 26.7 (5.8) years
Sex I: 48/52 (92.3%) M C: 55/60 (91.6%) M
Groups comparable at baseline? Yes. The groups showed no significant differences regarding baseline characteristics as shown in Table 1. |
Describe intervention (treatment/procedure/test):
Short description: operative treatment with arthroscopic shoulder stabilization.
Detailed description: Patients underwent surgery within 3 weeks after trauma. Surgeries were performed with patients in the lateral decubitus position, and 3 portals were used. A standardized arthroscopic shoulder stabilization procedure was performed with labral repair and capsular shift using a knotless technique. For refixation of the labrum, at least 3 PEEK anchors with an FiberWire loop (Arthrex) were used. Postoperatively, the patients were immobilized in internal rotation in a sling for 3 weeks, and a standardized rehabilitation protocol was performed.
|
Describe control (treatment/procedure/test):
Short description: Nonoperative treatment.
Detailed description: Immobilization in 60 degrees of external rotation and 30 degrees of abduction. For immobilization in the external rotation plus abduction position, a Bledsoe ARC XR orthosis was used. The immobilization treatment began at least 3 days after trauma. Patients were instructed to wear the brace 24 hours a day, for 3 weeks in total. |
Length of follow-up: Two years.
Loss-to-follow-up: Intervention: N = 8 (15.4%) Reasons: all 8 patients were lost to follow-up because contact information changed without notice.
*Baseline characteristics of the patients lost to follow-up or excluded due to non-compliance did not differ from the characteristics of the other patients. N = 13 (21.7%) Reasons: 4 patients dropped out of the study because of non-compliance (ie, they interrupted the immobilization treatment) and 9 patients were lost to follow-up because contact information changed without notice.
Control: N = 13 (21.7%) Reasons: 4 patients dropped out of the study because of non-compliance (ie, they interrupted the immobilization treatment) and 9 patients were lost to follow-up because contact information changed without notice.
*Baseline characteristics of the patients lost to follow-up or excluded due to non-compliance did not differ from the characteristics of the other patients.
|
Outcome 1: overall recurrence rate of instability, n/N (%) I: 1/44 (2.3%) C: 9/47 (19.1%)
*recurrent instability was further divided in traumatic and atraumatic events.
Traumatic I: 1/1 (100%) C: 5/9 (55.6%)
Atraumatic I: 0/1 (0%) C: 4/9 (44.4%)
Traumatic and atraumatic events were further divided in subluxations and dislocations.
Traumatic subluxation I: 1/1 (100%) C: 1/5 (20.0%) Traumatic dislocation I: 0/1 (0%) C: 4/5 (80.0%)
Atraumatic subluxation I: 0/1 (0%) C: 2/4 (50.0%)
Atraumatic dislocation I: 0/1 (0%) C: 2/4 (50.0%)
Outcome 2: need for (secondary) surgery, n/N (%) I: 0/44 (0%) C: 5/47 (10.6%)
*additional surgery was secondary arthroscopic shoulder stabilization due to recurrent shoulder instability at a mean of 12.2 months (range 5 to 21 months) after initial dislocation.
Outcome 3: complications, n/N (%) I: 0/44 (0%) C: 0/47 (0%)
Outcome 4: shoulder instability symptoms among patients who did not have a recurrent instability event
Positive apprehension test, n/N (%) I: 2/44 (4.7%) C: 3/47 (7.9%)
Outcome 5: range of motion
External rotation at 90 degrees of abduction, mean (SD) I: 80 (12.0) degrees C: 86 (9.0) degrees
Outcome 6: patients reported outcomes
WOSI-score, mean (SD) I: 92.7% (8.1) C: 91.5% (7.9)
Rowe-score, mean (SD) I: 88.5 (11.2) points C: 89.1 (7.1) points
Constant-Murley score, mean (SD) I: 93.9 (10.1) points C: 96.9 (4.7) points
Subjective Shoulder Value, mean (SD) I: 93.1% (6.5) C: 93.6% (4.4)
|
Author’s conclusion: Immobilization in ER1ABD versus primary arthroscopic shoulder stabilization for the treatment of FSD showed no differences in clinical shoulder scores. However, recur- rent instability was significantly higher after nonoperative treatment. Traumatic as well as atraumatic recurrent instability events can be observed, which mainly affect patients younger than 30 years who are active in sports. Primary operative stabilization might be preferred for this group if the patient desires the lowest risk for recurrent dislocation.
|
|
Pougès (2021) |
Type of study: Controlled, prospective, randomized trial.
Setting and country: Emergency department of a hospital. France.
Funding: Not reported.
Conflicts of interest: The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
|
Inclusion criteria:
Exclusion criteria:
N total at baseline: Intervention: N=20 Control: N=20
Important prognostic factors2: Age, mean (SD) / median (IQR) I: 22 (20.5 to 22.5) C: 21.5 (20 to 22.5) P=0.63
Sex I: 15/20 (75%) M C: 18/20 (90%) M P=0.41
Groups comparable at baseline? Yes.
|
Describe intervention (treatment/procedure/test):
Short description: operative treatment.
Detailed description: Patients under- went arthroscopic Bankart repair surgery. Surgery was to be performed in the 15 days after the first episode of ASD. Internal rotation immobilization was to be followed for the first 3 weeks after the surgery.
* Physical therapy began at 3 weeks postoperatively and consisted of passive and active mobilization while limiting external rotation to 30° and abduction to 90°. Unlimited range of motion was allowed after 6 weeks.
|
Describe control (treatment/procedure/test):
Short description: Nonoperative treatment.
Detailed description: Patients were immobilized for 3 weeks after ASD.
*Physical therapy began at 3 weeks and consisted of passive and active mobilization while limiting external rotation to 30° and abduction to 90°. Unlimited range of motion was allowed after 6 weeks.
|
Length of follow-up: Two years.
Loss-to-follow-up: Intervention: N = 0
Control: N = 0
|
Outcome 1: overall recurrence rate of shoulder instability, n/N (%) I: 2/20 (10.0%) C: 14/20 (70.0%)
Of the 14 patients in the nonoperative treatment group, 13 described subluxations and 6 had complete dislocations requiring reduction by a third person. The last patient had a positive apprehension test. Fewer patients in the operative treatment group versus the nonoperative group had another episode of dislocation (0 vs 6), subluxation (2 vs 13), or a positive apprehension test (1 vs 11).
Outcome 2: need for (secondary) surgery, n/N (%) I: 1/20 (5.0%) C: 4/20 (20.0%)
Outcome 3: patient reported outcomes
WOSI-score, mean (SD) I: 11.5 (18.6) C: 17.7 (18.4)
Walch-Duplay score, mean (SD) I: 88.4 (19.3) C: 70.3 (30.7)
QuickDASH score, mean (SD) I: 6.5 (10.6) C: 11.2 (13.0)
Outcome 4: range of motion
Anterior elevation, mean difference with opposite side after two years I: -0.5 (2.3) degrees C: 2.1 (7.1) degrees
Abduction, mean difference with opposite side after two years I: 0.5 (2.3) degrees C: 5.8 (11.7) degrees
Extension, mean difference with opposite side after two years I: 3.2 (8.2) degrees C: 2.1 (7.9) degrees
External rotation at 0 degrees of abduction, mean difference with opposite side after two years I: -1.5 (6.7) degrees C: 3.7 (7.0) degrees
External rotation at 90 degrees of abduction, mean difference with opposite side after two years I: 0.5 (5.2) degrees C: 3.1 (8.2) degrees
Internal rotation, mean difference with opposite side after two years I: 19.0 (NR) degrees C: 19.0 (NR) degrees
Outcome 5: return to sport I: 95% (19/20) C: 68%
Outcome 6: Patient satisfaction Patients were asked, ‘‘After this first dislocation, would you agree to have (another) surgery now that you know the outcome?’’, n/N who answered ‘yes’ I: 17/20 (85.0%) C: 7/20 (35%)
*8 patients in the nonoperative treatment group had no opinion, 4 patients would not have operative treatment, and 1 patient was lost to follow-up and did not respond. |
Author’s conclusion: This study showed that arthroscopic Bankart repair after the first episode of ASD offers better results than nonoperative treatment in terms of risk of recurrence and functional results while preserving range of motion. In light of these results, arthroscopic Bankart repair could be offered as a primary treatment after the first episode of ASD in patients younger than 25 years. A longer follow-up will be necessary to confirm the durability of these findings.
|
Risk of bias tabel
Systematic review(s)
|
Study
First author, year |
Appropriate and clearly focused question?1
Yes/no/unclear |
Comprehensive and systematic literature search?2
Yes/no/unclear |
Description of included and excluded studies?3
Yes/no/unclear |
Description of relevant characteristics of included studies?4
Yes/no/unclear |
Appropriate adjustment for potential confounders in observational studies?5
Yes/no/unclear/not applicable |
Assessment of scientific quality of included studies?6
Yes/no/unclear |
Enough similarities between studies to make combining them reasonable?7
Yes/no/unclear |
Potential risk of publication bias taken into account?8
Yes/no/unclear |
Potential conflicts of interest reported?9
Yes/no/unclear |
|
Lu (2019) |
Yes |
Yes |
Yes |
Yes |
Not applicable |
Yes |
Yes |
Yes |
Yes |
Randomized controlled trial(s)
|
Study reference
(first author, publication year) |
Was the allocation sequence adequately generated?
Definitely yes Probably yes Probably no Definitely no |
Was the allocation adequately concealed?
Definitely yes Probably yes Probably no Definitely no |
Blinding: Was knowledge of the allocated interventions adequately prevented?
Definitely yes Probably yes Probably no Definitely no |
Was loss to follow-up (missing outcome data) infrequent?
Definitely yes Probably yes Probably no Definitely no |
Are reports of the study free of selective outcome reporting?
Definitely yes Probably yes Probably no Definitely no |
Was the study apparently free of other problems that could put it at a risk of bias?
Definitely yes Probably yes Probably no Definitely no |
Overall risk of bias If applicable/necessary, per outcome measure
LOW Some concerns HIGH
|
|
Bottoni (2002) |
Definitely yes
Reason: Patients who voluntarily entered the study were randomized to one of two groups by using the last digit of their social security numbers
|
Probably no
Reason: randomized by using the last digit of their social security numbers; that is, patients with odd numbers were assigned to the operative group.
|
Definitely no.
Reason: blinding of patients and study personnel was not possible.
|
Probably no.
Reason: three out of twelve (25%) patients were lost to follow-up but all in the operative treatment group
|
Probably yes.
Reason: all predefined outcome measures were reported. |
No information.
Reason: study does not describe any other problems.
|
Some concerns/high
Reason: no blinding possible and high percentage lost to follow-up in the operative treatment group.
|
|
Jakobsen (2007) |
Definitely yes.
Reason: the patients were randomized via a sealed-envelope technique to either open Bankart repair or non-operative treatment.
|
No information.
Reason: -
|
Probably no.
Reason: Blinding of patients was not possible. Blinding of study personnel not mentioned.
|
Probably yes.
Reason: only one patient (in the operative group) could not be tracked.
|
Probably yes.
Reason: all predefined outcome measures were reported. |
Probably yes.
Reason: One of the weaknesses of the study is that it was performed as a multicenter study with several surgeons. We tried to reduce the disadvantages by gathering all experienced surgeons before the study was begun and teaching everyone the arthroscopic evaluation system, the Constant score measures, and the operative technique in a cadaver laboratory. The 10- year evaluation was performed as a telephone inter- view, which did not give us the opportunity to examine range of motion or any signs of osteoarthritis.
|
Some concerns
Reason: unclear allocation concealment and no blinding.
|
|
Kirkley (2005)
|
Definitely yes.
Reason: it was decided to stratify the randomization based on age: (1) 22 years or younger and (2) 23 to 30 years of age. The randomization was also stratified for the surgeon to eliminate the bias that may be introduced by small differences in surgical technique. Each surgeon was provided with a set of opaque envelopes, each of which contained group assignment as generated by a computer program using variable block sizes of 2 and 4.
|
No information.
Reason: -
|
Definitely no.
Reason: no blinding of participants possible.
|
Probably yes.
Reason: Thirty-three of the 40 original subjects were found and contacted by telephone; 31 agreed to be evaluated and returned questionnaire data, 16 from the operative treatment group and 15 from the traditional treatment group.
|
Probably yes.
Reason: all predefined outcome measures were reported. |
No information.
Reason: -
|
Some concerns.
Reason: no blinding and unclear allocation concealment.
|
|
Minkus (2021) |
Definitely yes.
Reason: Patients were assigned to the nonoperative treatment with immobilization or the operative treatment with shoulder sta- bilization within 3 days after trauma and dislocation at a 1:1 allocation ratio
|
Definitely yes.
Reason: allocation ratio based on an allocation sequence that was generated on a computer and internet-based randomization tool.
|
Definitely no.
Reason: blinding of the patients was not possible and blinding of the outcome examiners was not feasible. This lack of blinding also creates a risk of bias.
|
Probably no
Reason: The number of patients who were lost because they refused to participate, sought treatment .3 days after dislocation, or had concomitant lesions listed under the exclusion criteria is unclear, leading to a potential selection bias.
Unfortunately, we were not able to conduct follow-up exami- nations of the patients who experienced a recurrent insta- bility and had to be excluded because of noncompliance. This compromises the analysis of clinical outcomes between the 2 groups because only patients who were successfully treated are considered in the 24-month follow-up results. An intention-to-treat analysis for patients who underwent operative stabilization secondarily was not performed.
|
Probably yes.
Reason: all predefined outcome measures were reported. |
Apart from the limitations named earlier, probably yes.
Reason: see previous sections. |
Some concerns/high
Reason: loss to follow-up was frequent, no blinding of study personnel (patient blinding was not possible). |
|
Pougès (2021) |
Definitely yes.
Reason: After providing con- sent, the patients were randomized to 1 of the 2 groups by opening envelopes prepared by the clinical research department, which were opened in a predetermined order.
|
Probably yes.
Reason: The investigators discovered the treatment group only when the patient was included in the study.
|
Definitely no
Reason: blinding of participants was not possible. Study personnel was also not blinded. |
Definitely yes.
Reason: 2 patients were lost to follow-up, but equally distributed over both groups. |
Probably yes.
Reason: all predefined outcome measures were reported. |
No information.
Reason: - |
Some concerns
Reason: no blinding of participants or personnel. |
|
Yapp (2020) |
Definitely yes.
Reason: Subjects were randomized to receive either an arthroscopic washout (AWO) or ABR
|
Probably yes.
Reason: Treatment allocation was concealed unless the patient experienced recurrent insta- bility requiring further investigation and treatment.
|
Probably yes.
Reason: Patients and data reviewers were blinded to the treatment allocation during the course of this study.
|
Probably yes.
Reason: high percentages of lost to follow-up in both groups but almost equal in both groups (30% in non-operative group and 25% in operative group).
|
Probably yes.
Reason: all predefined outcome measures were reported. |
Probably yes.
Reason: In the present trial, 3 patients died and another 20 patients (23%) were considered lost to follow-up following initial ran- domization. Although the loss to follow-up could lead to reporting bias, no differences were noted with respect to the age, sex, or number of high-risk patients in each cohort of patients who did not complete follow-up. No differences were found in the rate of recurrent dislocation or PROM scores measured at 2 years between those included in this long-term study and those who were excluded after 2 years.
|
Low/some concerns.
Reason:
|
Exclusie tabel
|
Systematic reviews |
|
|
Author and year |
Reason for exclusion |
|
Adam (2018) |
Includes the same studies as a more recent systematic review of van Spanning (2021). |
|
Brophy (2009) |
Includes the same studies as a more recent systematic review of van Spanning (2021). |
|
Chahal (2012) |
Includes the same studies as a more recent systematic review of van Spanning (2021). |
|
Godin (2010) |
Includes the same studies as a more recent systematic review of van Spanning (2021). |
|
Handoll (2004) |
Includes the same studies as a more recent systematic review of van Spanning (2021). |
|
Hurley (2020) |
Includes the same studies as a more recent systematic review of van Spanning (2021). |
|
Kavaja (2018) |
Includes the same studies as a more recent systematic review of van Spanning (2021). |
|
Longo (2014) |
Includes the same studies as a more recent systematic review of van Spanning (2021). |
|
Kraeutler (2020) |
Includes the same studies as a more recent systematic review of van Spanning (2021). |
|
Zaremski (2016) |
Includes the same studies as a more recent systematic review of van Spanning (2021). |
|
Randomized controlled trials |
|
|
Multanen (2020) |
Wrong comparison. |
|
2019 SFA Annual Meeting Abstracts |
Wrong study design. |
Beoordelingsdatum en geldigheid
Publicatiedatum : 14-12-2023
Beoordeeld op geldigheid : 13-10-2023
Algemene gegevens
De ontwikkeling/herziening van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd uit de Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Doel en doelgroep
Deze richtlijn bevat nuttige informatie voor alle zorgverleners die betrokken zijn bij de in de eerste-, tweede- en derdelijns zorg voor patiënten met een primaire, acute schouderluxatie.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2021 een multidisciplinaire werkgroep ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van de werkgroep) die betrokken zijn bij de zorg voor patiënten met een acute, primaire schouderluxatie.
Werkgroep
- Dhr. dr. R.J. (Robert Jan) Derksen (voorzitter), traumachirurg, Nederlandse Vereniging voor Heelkunde
- Dhr. dr. S.D. (Stijn) Nelen, traumachirurg, Nederlandse Vereniging voor Heelkunde
- Dhr. dr. N.W.L. (Niels) Schep, traumachirurg, Nederlandse Vereniging voor Heelkunde
- Mw. MSc. F. (Femke) Boon, fysio- en manueeltherapeut, Koninklijk Nederlands Genootschap voor Fysiotherapie
- Mw. MSc. K.M.C. (Karin) Hekman, fysio- en manueeltherapeut, Koninklijk Nederlands Genootschap voor Fysiotherapie
- Dhr. dr. O.A.J. (Olivier) van der Meijden, orthopedisch chirurg, Nederlandse Orthopaedische Vereniging
- Dhr. prof. Dr. M.P.J. (Michel) van den Bekerom, orthopedisch chirurg, Nederlandse Orthopaedische Vereniging
- Dhr. dr. D.N. (David) Baden, spoedeisende hulparts, Nederlandse Vereniging voor Spoedeisende Hulp Artsen
- Dhr. MA. T. (Thomas) Jonkergouw, adviseur patiëntbelang, Patiëntenfederatie Nederland
- Mw. M.G. (Maike) Broere, adviseur patiëntbelang, Patiëntenfederatie Nederland
- Mw. drs. L.E. (Louise) Huygen, radioloog, Nederlandse Vereniging voor Radiologie
Meelezers
- Dhr. drs. T. (Tjerk) de Ruiter, revalidatiearts, Nederlandse Vereniging van Revalidatieartsen
- Dhr. R.P.G. (Ramon) Ottenheijm, huisarts, Nederlands Huisartsen Genootschap
- Dhr. B.M.F. (Bart) van der Leeuw, anesthesioloog, Nederlandse Vereniging voor Anesthesiologie
Met ondersteuning van:
- Mw. dr. A.C.J. (Astrid) Balemans, adviseur, Kennisinstituut van Medisch Specialisten
- Dhr. MSc. M. (Mitchel) Griekspoor, adviseur, Kennisinstituut van Medisch Specialisten
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle werkgroepleden hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een module worden wijzigingen in belangen aan de voorzitter doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase.
Een overzicht van de belangen van werkgroepleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
|
Werkgroeplid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Dhr. dr. R.J. (Robert Jan) Derksen |
Traumachirurg |
ATLS-instructeur, stichting ALSG, 2-3 keer per jaar faculty-lid van een ATLS trauma-opvang cursus. Dit is een betaalde functie.
Bestuurslid Nederlandse Vereniging voor Traumachirurgie.
|
Persoonlijke financiële belangen Geen.
Persoonlijke relaties Geen.
Extern gefinancierd onderzoek Als ziekenhuis ontvangen wij een unrestricted educational grant van Mathys Medical. Hiermee bekostigen wij een arts-onderzoeker die onderzoek doet naar de eventuele meerwaarde van een schouderprothese in het geval van een complexe proximale humerusfractuur. Dit onderzoek is een joint-venture met het AUMC.
De uitkomsten van deze richtlijncommissie zullen geen voor- of nadelen met zich meebrengen voor de financier, de behandeling van een schouderluxatie is namelijk vrijwel nooit een prothese (uitgezonderd in zeldzame gevallen de luxatiefractuur).
Intellectuele belangen en reputatie Geen.
Overige belangen Geen. |
Geen restrictie.
|
|
Dhr. dr. S.D. (Stijn) Nelen
|
Traumachirurg |
ATLS-instructeur, betaald |
Persoonlijke financiële belangen Geen.
Persoonlijke relaties Geen.
Extern gefinancierd onderzoek Geen.
Intellectuele belangen en reputatie Geen.
Overige belangen Geen.
|
Geen restrictie.
|
|
Dhr. dr. N.W.L. (Niels) Schep
|
Traumachirurg |
Bestuurslid NED Ver Handchirurgie onbetaald Bestuurslid Big Hand Event onbetaald Instructeur Dutch Wrist Ascopie course onbetaald. Consultant Synthes, Arthrex: betrokken bij cursussen betaald. Chairman diverse AO cursussen onkosten vergoeding Instructeur IBRA course onkosten vergoeding. Instructeur CASH cursus, handfracturen onkostenvergoeding. Editor boek Leidraad chirurgie co- assistent revenuen geen. Instructeur ATLS |
Persoonlijke financiële belangen Geen.
Persoonlijke relaties Mijn echtgenote heeft een medisch congres bureau. Echter ik zie geen relatie met deze richtlijn.
Extern gefinancierd onderzoek Geen.
Intellectuele belangen en reputatie Diverse Zonmw beurzen voor onderzoek naar handfracturen. Ik heb diverse publicaties op het gebied van schouderstabilisatie, die wellicht in de richtlijn aan bod zullen komen.
Overige belangen Geen.
|
Geen restrictie.
De cursussen die voor arthrex worden gegeven gaan alleen over de hand en pols. Synthes levert geen producten die bij chirurgie bij schouderluxatie worden gebruikt. |
|
Mw. MSc. F. (Femke) Boon
|
Fysio- en manueeltherapeut |
Geen. |
Persoonlijke financiële belangen Werkzaam bij Schoudercentrum IBC Amstelland.
Persoonlijke relaties Geen.
Extern gefinancierd onderzoek Geen.
Intellectuele belangen en reputatie Geen.
Overige belangen Geen. |
Geen restrictie.
|
|
Mw. MSc. K.M.C. (Karin) Hekman
|
Fysio- en manueeltherapeut |
Bestuurslid SchouderNetwerken Nederland, onbetaald. |
Persoonlijke financiële belangen Geen.
Persoonlijke relaties Geen.
Extern gefinancierd onderzoek ZonMw Shoulder Innovation, 1,5 lijn schouderzorg (rol als projectleider)
ZonMw schouderspreekuur opzet in de 1e lijn (rol als projectleider).
Intellectuele belangen en reputatie In mijn werkveld is schouderinstabiliteit een van mijn interessegebieden. Ik behandel veel patiënten met schouderinstabiliteit, participeer in (tot op heden nog niet gefinancierde) onderzoeken om de kwaliteit van zorg te verbeteren.
Overige belangen Geen. |
Geen restrictie.
|
|
Dhr. dr. O.A.J. (Olivier) van der Meijden
|
Orthopedisch chirurg |
Geen. |
Persoonlijke financiële belangen Geen.
Persoonlijke relaties Geen.
Extern gefinancierd onderzoek Geen.
Intellectuele belangen en reputatie Geen.
Overige belangen Geen.
|
Geen restrictie.
|
|
Dhr. prof. Dr. M.P.J. (Michel) van den Bekerom
|
Orthopaedisch chirurg |
Orthopedisch Expertise Centrum Amsterdam Orthopedisch chirurgische expertisen vooral op het gebied van letselschade en arbeidsongeschiktheid Betaalde functies. Voornemens een fellowship te starten dus een vervolgopleiding op schouder/elleboog gebied voor een orthopedisch chirurg. Dit fellowship wordt dan mede (financieel) ondersteund door een firma die materiaal maakt dat we gebruiken bij schouderstabilisaties. Het betreft een overeenkomst tussen het OLVG en deze firma. Ik zal geen geld op persoonlijke titel ontvangen en het bedrag is ook niet afhankelijk van aantal operaties dat we verrichten. Het fellowship en dus de overeenkomt hebben een louter educatief doel. |
Persoonlijke financiële belangen Geen.
Persoonlijke relaties Geen.
Extern gefinancierd onderzoek Geen.
Intellectuele belangen en reputatie Geen.
Overige belangen (Betaald) onderwijs geven IOC NPI Amersfoort SOMT Amersfoort. |
Geen restrictie.
Er wordt een fellow aangenomen, mede bekostigd door een bedrijf. De overeenkomst is tussen het bedrijf en het OLVG, Van den Bekerom heeft hier zelf geen persoonlijk financieel belang bij. |
|
Dhr. dr. D.N. (David) Baden
|
Spoedeisende Hulp Arts |
Voorzitter NVSHA-vacatiegelden Voorzitter expertgroep "Met spoed beschikbaar" |
Persoonlijke financiële belangen Geen.
Persoonlijke relaties Geen.
Extern gefinancierd onderzoek
Intellectuele belangen en reputatie Geen.
Overige belangen Geen.
|
Geen restrictie.
|
|
Dhr. MA. T. (Thomas) Jonkergouw
|
Adviseur patiëntbelang |
Vrijwilliger Diabetes Vereniging Nederland - onbetaald. Organisatie van zomerkampen voor kinderen. |
Persoonlijke financiële belangen Geen.
Persoonlijke relaties Geen.
Extern gefinancierd onderzoek Geen.
Intellectuele belangen en reputatie Geen.
Overige belangen Geen.
|
Geen restrictie.
|
|
Mw. drs. L.E. (Louise) Huygen
|
Radioloog |
Geen. |
Persoonlijke financiële belangen Geen.
Persoonlijke relaties Geen.
Extern gefinancierd onderzoek Geen.
Intellectuele belangen en reputatie Geen. |
Geen restrictie.
|
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door het uitnodigen van de Patiëntenfederatie Nederland voor de schriftelijke knelpuntenanalyse en deelname van een afgevaardigde van de Patiëntenfederatie Nederland in de werkgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptmodules zijn tevens voor commentaar voorgelegd aan de Patiëntenfederatie Nederland en de eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Implementatie
|
Aanbeveling |
Tijdspad voor implementatie: 1 tot 3 jaar of > 3 jaar |
Verwacht effect op kosten |
Randvoorwaarden voor implementatie (binnen aangegeven tijdspad) |
Mogelijke barrières voor implementatie1 |
Te ondernemen acties voor implementatie2 |
Verantwoordelijken voor acties3 |
Overige opmerkingen |
|
Alle aanbevelingen |
1 tot 3 jaar |
Geen verwacht effect op indirecte kosten. Effect op directe kosten van individuele patiënt kunnen mogelijk hoger worden. |
Geen. |
Geen. |
Promoten richtlijn schouderluxaties. Klinische les NTvG. Webinar vanuit de NVT. |
Werkgroepleden en Kennisinstituut. Werkgroep. NVT. |
Geen. |
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 2.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Knelpuntenanalyse en uitgangsvragen
Tijdens de voorbereidende fase inventariseerde de werkgroep de knelpunten in de zorg voor patiënten die een schouderluxatie ervaren. Tevens zijn er knelpunten aangedragen door middel van een schriftelijke knelpuntenanalyse. Een verslag hiervan is opgenomen onder aanverwante producten.
Op basis van de uitkomsten van de knelpuntenanalyse zijn door de werkgroep concept-uitgangsvragen opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvraag behorende bij de uitgangsvraag inventariseerde de werkgroep welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. Hierbij werd een maximum van acht uitkomstmaten gehanteerd. De werkgroep waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerde de werkgroep tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur is te vinden onder ‘Zoeken en selecteren’ onder Onderbouwing. Indien mogelijk werd de data uit verschillende studies gepoold in een random-effects model. Review Manager 5.4 werd gebruikt voor de statistische analyses. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie http://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding).
GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
|
GRADE |
Definitie |
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in richtlijnen volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE methodiek.
Formuleren van aanbevelingen
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door de werkgroep wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. De werkgroep heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
In de knelpuntenanalyse en bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen. Meer algemene, overkoepelende, of bijkomende aspecten van de organisatie van zorg worden behandeld in de module Organisatie van zorg.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd aan de betrokken (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd ter commentaar. De commentaren werden verzameld en besproken met de werkgroep. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door de werkgroep. De definitieve richtlijnmodule werd aan de deelnemende (wetenschappelijke) verenigingen en (patiënt) organisaties voorgelegd voor autorisatie en door hen geautoriseerd dan wel geaccordeerd.
Zoekverantwoording
Algemene informatie
|
Richtlijn: Schouderluxaties |
|
|
Uitgangsvraag: Wat is de waarde van chirurgische interventie bij een primaire anterieure schouderluxatie? |
|
|
Database(s): Ovid/Medline, Embase |
Datum: 10-02-2022 (update 17-03-2022) |
|
Periode: 1990 - heden |
Talen: Engels, Nederlands |
|
Literatuurspecialist: Miriam van der Maten |
|
|
BMI zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Bij gebruikmaking van een volledig zoekblok zal naar de betreffende link op de website worden verwezen. |
|
|
Toelichting: Voor deze vraag is gezocht op de elementen:
De sleutelartikelen van De Carli, Bottoni, Kirkley en Jakobsen worden gevonden met de zoekopdracht. De sleutel artikelen van Larrain, Arciero, Gigis, en Shih, worden wel gevonden met de zoekterminologie, maar vallen uit de zoekopdracht op basis van studiedesign (geen SR of RCT). Er werd eerste gezocht naar SR. Op basis daarvan werd de review van Spanning (2021) als basis genomen voor de module. Vanaf de zoekdatum van die search, is nog aanvullend naar RCT gezocht (17 maart 2022) |
|
|
Te gebruiken voor richtlijnen tekst: In de databases Embase en Ovid/Medline is op 10 februari 2022 (update RCT 17 maart 2022) met relevante zoektermen gezocht naar systematische reviews en RCT over de waarde van chirurgische interventie bij een primaire anterieure schouderluxatie.De zoekopdracht leverde 98 resultaten op. |
|
Zoekopbrengst
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SRs |
79 |
67 |
88 |
|
RCT vanaf 2020 |
12 |
8 |
10 |
|
Totaal |
|
|
98 |
Zoekstrategie
Embase
|
No. |
Query |
Results |
|
#18 |
#14 AND #16 NOT #17 AND [01-04-2020]/sd = RCT vanaf April 2020 |
12 |
|
#17 |
#14 AND #15 = SR |
79 |
|
#16 |
'randomized controlled trial'/exp OR random*:ti,ab OR (((pragmatic OR practical) NEAR/1 'clinical trial*'):ti,ab) OR ((('non inferiority' OR noninferiority OR superiority OR equivalence) NEAR/3 trial*):ti,ab) OR rct:ti,ab,kw |
1873986 |
|
#15 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
733409 |
|
#14 |
#11 AND #12 AND #13 AND ([english]/lim OR [dutch]/lim) AND [1990-2022]/py NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
1104 |
|
#13 |
'conservative treatment'/exp/mj OR conservative:ti,ab,kw OR noninvasive:ti,ab,kw OR 'non invasive':ti,ab,kw OR nonsurg*:ti,ab,kw OR 'non surg*':ti,ab,kw OR nonoperati*:ti,ab,kw OR 'non operati*':ti,ab,kw OR expectative*:ti,ab,kw OR 'watchful waiting':ti,ab,kw OR 'immobilization'/exp OR immobili*:ti,ab,kw OR 'physiotherapy'/exp OR physiotherap*:ti,ab,kw OR 'physio therap*':ti,ab,kw OR 'physical therap*':ti,ab,kw OR 'kinesiotherapy'/exp OR kinesiotherap*:ti,ab,kw OR kinesitherapeutic*:ti,ab,kw OR 'occupational therapy'/exp OR 'occupation* therap*':ti,ab,kw OR ergotherapy*:ti,ab,kw |
1085871 |
|
#12 |
'surgery'/exp/mj OR 'surgery'/lnk OR surgic*:ti,ab,kw OR surger*:ti,ab,kw OR surgeon*:ti,ab,kw OR operation*:ti,ab,kw OR operative:ti,ab,kw OR invasive:ti,ab,kw OR restorati:ti,ab,kw OR 'bankart repair'/exp OR bankart*:ti,ab,kw OR (('rotator cuff' NEAR/3 repair*):ti,ab,kw) OR 'arthroscopic stabili*ation':ti,ab,kw |
6174595 |
|
#11 |
'shoulder dislocation'/exp/mj OR (((shoulder* OR glenohumeral) NEAR/5 (dislocat* OR luxat* OR instab*)):ti,ab,kw) |
10684 |
Ovid/Medline
|
# |
Searches |
Results |
|
9 |
(5 and 7) not 8 andt dt=20200401-20220401 =RCT vanaf April 2020 |
8 |
|
8 |
5 and 6 = SR |
67 |
|
7 |
(exp randomized controlled trial/ or randomized controlled trials as topic/ or random*.ti,ab. or rct?.ti,ab. or ((pragmatic or practical) adj "clinical trial*").ti,ab,kf. or ((non-inferiority or noninferiority or superiority or equivalence) adj3 trial*).ti,ab,kf.) not (animals/ not humans/) |
1351271 |
|
6 |
(meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf.) not (comment/ or editorial/ or letter/ or ((exp animals/ or exp models, animal/) not humans/)) |
546853 |
|
5 |
limit 4 to ((english language or dutch) and yr="1990 -Current") |
834 |
|
4 |
1 and 2 and 3 |
1126 |
|
3 |
exp Conservative Treatment/ or exp Immobilization/ or immobili*ation.ti,ab,kf. or immobili*e.ti,ab,kf. or conservative.ti,ab,kf. or noninvasive.ti,ab,kf. or 'non invasive'.ti,ab,kf. or nonsurg*.ti,ab,kf. or 'non surg*'.ti,ab,kf. or nonoperati*.ti,ab,kf. or 'non operati*'.ti,ab,kf. or expectative*.ti,ab,kf. or 'watchful waiting'.ti,ab,kf. or exp Physical Therapy Modalities/ or exp Occupational Therapy/ or physiotherap*.ti,ab,kf. or 'physio therap*'.ti,ab,kf. or 'physical therap*'.ti,ab,kf. or kinesiotherap*.ti,ab,kf. or kinesitherapeutic*.ti,ab,kf. or 'occupation* therap*'.ti,ab,kf. or ergotherapy*.ti,ab,kf. |
651279 |
|
2 |
exp Specialties, Surgical/ or su.fs. or surgic*.ti,ab,kf. or surger*.ti,ab,kf. or surgeon*.ti,ab,kf. or operation*.ti,ab,kf. or operative.ti,ab,kf. or invasive.ti,ab,kf. or restorati.ti,ab,kf. or Bankart*.ti,ab,kf. or ('rotator cuff' adj3 repair*).ti,ab,kf. or 'arthroscopic stabili*ation'.ti,ab,kf. |
3979903 |
|
1 |
exp Shoulder Dislocation/ or ((shoulder* or glenohumeral) adj5 (dislocat* or luxat* or instab*)).ti,ab,kf. |
10209 |