Behandeling van simpele appendicitis bij volwassenen
Uitgangsvraag
Welke behandeling heeft de voorkeur bij volwassen patiënten die zich presenteren met acute simpele appendicitis?
Aanbeveling
Maak in het geval van een appendicitis, zonder kenmerken van een complexe appendicitis of sepsis, duidelijk aan de patiënt dat er mogelijkheid is tot verschillende behandelopties: conservatieve behandeling of appendectomie.
Overweeg een conservatieve behandeling met antibiotica* bij volwassen patiënten met acute appendicitis, zonder kenmerken van complexe appendicitis of sepsis, als step-up mogelijkheid binnen de behandeling.
Deze voorkeur stelt de arts vast door middel van gedeelde besluitvorming met de patiënt, waarbij:
-
- De voor- en nadelen van beide behandelingen worden besproken met de patiënt waarbij de kans op het alsnog moeten ondergaan van een appendectomie in het eerste jaar bij hooguit een derde van de patiënten aan de orde is maar de kans op complicaties – ook bij latere appendectomie – vergelijkbaar is;
- De arts de patiënt helpt om de afwegingen te maken afhankelijk van wat belangrijk is voor de patiënt.
Wees terughoudend met een conservatieve behandeling indien een faecoliet/appendicoliet aanwezig is op beeldvorming.
*Volgens lokaal protocol voor abdominale infecties.
Overwegingen
Voor- en nadelen van de interventie en de kwaliteit van het bewijs
Er is literatuuronderzoek verricht naar de uitkomsten van conservatieve behandeling in vergelijking met appendectomie bij volwassen patiënten met acute, simpele appendicitis. Het aantal complicaties werd als cruciale uitkomstmaat gedefinieerd.
Appendicitis kan zich presenteren als simpele en complexe appendicitis. Simpele appendicitis wordt gedefinieerd als flegmoneuze appendicitis zonder necrose of perforatie, ook wel "ongecompliceerd" genoemd. Een complexe appendicitis omvat een gangreneuze ontsteking danwel een perforatie van de appendix of een appendicitis met een abces (Bhangu, 2015).
Deze variant is weinig progressief en mogelijk reversibel (Bhangu, 2015). Ondanks de lage bewijskracht lijkt het aantal complicaties niet te verschillen tussen volwassen patiënten die operatief of conservatief worden behandeld. Er is tevens gekeken naar het aantal patiënten dat na initiële conservatieve behandeling alsnog binnen een jaar of later een appendectomie moest ondergaan, vanwege het terugkeren van een appendicitis na een initieel ingezette conservatieve behandeling. Het percentage patiënten dat in eerste instantie conservatief werd behandeld en binnen een jaar alsnog een appendectomie moest ondergaan varieerde in de geïncludeerde studies tussen de 12.5% en 35.0%. In deze module werd een conservatieve behandeling vergeleken met behandeling middels een appendectomie, waardoor het aantal patiënten dat een appendectomieën onderging in de controlegroep automatisch 100% betrof. Hierdoor was het niet mogelijk om de literatuur te graderen en een GRADE-conclusie op te stellen.
In deze aanbeveling is een recidief of persisterende appendicitis waarvoor een appendectomie verricht moet worden niet als complicatie meegenomen. De conservatieve behandeling van een appendicitis wordt als een step-up behandeling gezien, waarbij in 12.5 tot 35.0% na een jaar alsnog een appendectomie uitgevoerd moet worden, afhankelijk van patiënt selectie. Bij patiënten met een appendicoliet heeft namelijk een conservatieve behandeling minder kans van slagen (50%) en diverse trials hebben deze patiënten niet uitgesloten van deelname.
Een appendicoliet (faecoliet) in de appendix, gezien op beeldvorming, is bij volwassenen geassocieerd met een hoge kans op het falen van conservatieve therapie en een hogere recidief kans (CODA collaborative, 2021; Mahida, 2016; Tanaka, 2015; Vons, 2011). Het lijkt dat deze groep minder geschikt is voor conservatieve therapie.
Op basis van de huidige literatuur kan, met een redelijke bewijskracht, worden gesteld dat een appendectomie bij volwassen patiënten met een simpele appendicitis leidt tot minder kans op heropnames. Kwaliteit van leven, gemeten van de EQ-5D, lijkt niet te verschillen tussen beide groepen, hoewel de bewijskracht voor kwaliteit van leven op ‘zeer laag’ werd gegradeerd. Verder zien we dat volwassen patiënten die conservatief behandeld zijn minder verzuim van werk ziektedagen lijken te hebben dan volwassen patiënten die werden behandeld middels appendectomie, maar ook hier is de bewijskracht zeer laag, wat inhoudt dat de literatuur zeer onzeker is en het gevonden effect mogelijk niet het werkelijke effect goed weerspiegelt. Wel lagen beide groepen even lang opgenomen in het ziekenhuis tijdens de behandeling van de appendicitis. Let wel, vanwege de grote heterogeniteit in gerapporteerde uitkomsten is de bewijskracht voor zowel de kwaliteit van leven als het aantal ziektedagen zeer laag, waardoor de resultaten hiervan met grote voorzichtigheid geïnterpreteerd dienen te worden. Gezien het ontbreken van onderzoek met voldoende bewijskracht om een uitspraak te doen over complicaties, opnameduur en kwaliteit van leven en ziekteverzuim tussen de verschillende behandelingen blijft operatieve behandeling tot op heden de gouden standaard.
Eén op één vergelijken van conservatieve therapie met een appendectomie is lastig; beide behandelingen brengen enerzijds risico’s en anderzijds voordelen met zich mee. De kans op recidief na een appendectomie is praktisch nihil wat het lastig vergelijkbaar maakt met conservatieve therapie. Daar staat tegenover dat patiënten die operatief worden behandeld, ondanks dat de literatuur in deze module onzeker is over het effect van een operatieve behandeling op het aantal complicaties, in z’n algemeenheid worden blootgesteld aan de risico’s die anesthesie en chirurgie met zich meebrengen, evenals de kans op algemene bijwerkingen na een operatieve behandeling. Aan de andere kant worden de risico’s die een toegenomen consumptie van antibiotica met zich meebrengt niet meegenomen in deze overweging, enerzijds omdat dit (nog) niet bekend is, anderzijds omdat dit niet gemeten is zoals bijwerkingen (adverse events) van de specifieke antibioticakuur. Een voorkeur voor één van beide behandelingen lijkt dan ook afhankelijk van de weging van de secundaire voor- en nadelen, welke moeten worden afgewogen aan de hand van individuele voorkeuren van de patiënt.
Inherent aan het conservatief behandelen van een appendicitis is dat er geen weefsel wordt verkregen voor histopathologisch onderzoek. Dit zou kunnen leiden tot het missen van een maligniteit in de appendix. Echter, in een recent gepubliceerd onderzoek van de Jonge (2023) werd onderzocht of het niet-routinematig uitvoeren van histopathologisch onderzoek leidt tot het missen van een maligniteit in de appendix. Uit de resultaten bleek dat een neoplasma van de appendix met klinische gevolgen zou zijn gemist in 22/4966 (0,4%) patiënten. In 5/22 (22.7%) patiënten werd restziekte volledig gereseceerd tijdens aanvullende operatieve behandeling. Dit zou betekenen dat in 1,01 op de 1000 patiënten (bovengrens 95% BI 1,61:1000) een neoplasma van de appendix met klinische gevolgen voor de patiënt gemist zou worden. Daarentegen zouden 10/22 (4.5%) van de patiënten niet zijn blootgesteld aan potentiële schade als gevolg van aanvullende resecties zonder duidelijk voordeel, terwijl de gevolgen noch gunstig of schadelijk waren in de resterende 7/22 (3.2%) van de patiënten. De Jonge (2023) concludeert daarmee dat selectief histopathologisch onderzoek na appendectomie voor het vermoeden op een appendicitis uit oncologisch oogpunt veilig is en mogelijk resulteert in een vermindering van de werklast van pathologen, minder kosten met zich meebrengt en leidt tot minder onnodige resecties zonder een duidelijk voordeel. Echter, het is nog onduidelijk hoe en of patiënten met een onderliggende maligniteit zouden reageren op conservatieve behandeling met antibiotica of dat preoperatieve diagnostiek al zal leiden tot exclusie van patiënten voor conservatieve behandeling.
Waarden en voorkeuren van patiënten (en evt. hun verzorgers)
De keuze van de behandeling is tevens voorkeursgevoelig en daarom is het aan te bevelen om in samenspraak met de patiënt, door middel van gezamenlijke besluitvorming, te besluiten of het passend is om de simpele appendicitis operatief of conservatief te behandelen. De arts maakt hierbij duidelijk dat er een keuze is tussen verschillende mogelijkheden, bespreekt de voor- en nadelen en helpt de patiënt om de afwegingen te maken afhankelijk van wat belangrijk is voor de patiënt. Zo kan de conservatie behandeling van appendicitis ook als een step-up behandeling aan de patiënt worden voorgelegd waarbij een eventuele appendectomie een vervolgstap is na een behandeling met antibiotica.
Kosten (middelenbeslag)
Voor volwassen is nog beperkt onderzoek gedaan naar kosten, maar er lijkt een kostenreductie voor de conservatieve behandeling (O’leary, 2021; Sippola, 2017). De kosten-batenanalyse van O’leary (2021) laat zien dat de gemiddelde kosten voor appendectomie significant hoger zijn dan de kosten voor een conservatieve behandeling, respectievelijk €4816,- versus €3077,- (p< 0.001). Wanneer er additionele interventies nodig waren voor de behandeling van een recidief bij conservatieve behandeling, waren de kosten gemiddeld €830,- hoger dan bij directe behandeling middels chirurgie. Kosteneffectiviteitsanalyses zullen moeten uitwijzen of conservatieve behandeling ook kosteneffectief is in vergelijking met chirurgische behandeling.
Rationale van de aanbeveling: weging van argumenten voor en tegen de interventies
Samenvattend laat de analyse van de beschikbare literatuur zien dat zowel een appendectomie als een conservatieve behandeling van een simpele appendicitis een goede behandeling is. Eén op één vergelijken van beide behandelingen is lastig. Ongeveer de helft van een ondervraagde sample van de bevolking en evenzo van patiënten die een appendectomie hebben ondergaan geeft de voorkeur aan een conservatieve behandeling, zelfs als de kans op alsnog een appendectomie hoog is.
De behandelaar moet samen met de patiënt een keuze maken welke behandeling op dat moment de voorkeur geniet. De meegenomen argumenten zijn de kans op het optreden van complicaties, heropname, opnameduur in het ziekenhuis, kwaliteit van leven, en verzuim van werk. Tevens moet de aanwezigheid van een faecoliet/appendicoliet worden meegenomen in de keuze van behandeling. De kans op het alsnog moeten ondergaan van een appendectomie is niet gezien als falen van de initieel gekozen behandeling met antibiotica maar zal als ‘step-up benadering’ gezien worden waarbij de kans op het slagen van de antibiotica behandeling tenminste 70% is gedurende het eerste jaar en de aan- of afwezigheid van een faecoliet de kans van slagen beïnvloedt.
Onderbouwing
Appendicitis kan zich presenteren als simpele en complexe appendicitis. Simpele appendicitis wordt gedefinieerd als flegmoneuze appendicitis zonder necrose of perforatie, ook wel "ongecompliceerd" genoemd. Een complexe appendicitis omvat een gangreneuze ontsteking danwel een perforatie van de appendix of een appendicitis met een abces (Bhangu, 2015). Hoewel chirurgie de standaardbehandeling is, ongeacht de presentatie, laten meerdere studies zien dat niet-operatieve opties kunnen worden toegepast bij simpele appendicitis (Livingston, 2011; Wagner, 2018). Een appendectomie is wereldwijd één van de meest uitgevoerde operatieve behandelingen, elke operatie gaat gepaard met risico's en complicaties, zoals onder andere postoperatieve infecties (Margenthaler, 2003; Sammalkorpi, 2018). In deze module wordt de effectiviteit en veiligheid van een niet-operatieve behandeling versus appendectomie voor acute simpele appendicitis bij volwassenen onderzocht. Er werd specifiek gekeken of de conservatieve behandeling toegevoegd kan worden aan het behandelpalet voor een simpele acute appendicitis.
Complications (critical)
|
Low GRADE |
There seems to be no difference in complications between adult patients who were conservatively treated versus patients who underwent appendectomy for acute, uncomplicated appendicitis.
Source: Ceresoli, 2019; CODA Collaborative, 2020; CODA Collaborative, 2021; Eriksson, 1995; Salminen, 2015; Styrud, 2006; Talan, 2017; Vons, 2011 |
Readmission (skewed by conservative step-up approach)
|
Moderate GRADE |
Conservative treatment is associated with an increase in readmission rate compared to appendectomy in adult patients with acute, uncomplicated appendicitis but readmission for appendectomy after conservative treatment as part of a step-up approach is not registered separately.
Source: Ceresoli, 2019; CODA Collaborative, 2020; Eriksson, 1995; Salminen, 2015 |
Length of hospital stay (important)
|
Low GRADE |
There seems to be no difference in length of hospital stay between adult patients who were conservatively treated versus patients who underwent appendectomy for acute, uncomplicated appendicitis.
Source: Ceresoli, 2019; CODA collaborative, 2020; Eriksson, 1995; O’Leary, 2021; Salminen, 2015; Salminen (2018); Styrud, 2006; Talan, 2017; Vons, 2011 |
Quality of life (important)
|
Very low GRADE |
The evidence is very uncertain about the effect of conservative treatment on quality of life in comparison with adult patients who underwent appendectomy for acute, uncomplicated appendicitis.
Sources: CODA Collaborative, 2020; O’leary, 2021; Talan, 2017. |
Days missed from work due to sickness (important)
|
Very low GRADE |
The evidence is very uncertain about the effect of conservative treatment on the number of days missed from work due to sickness in comparison with adult patients who underwent appendectomy for acute, uncomplicated appendicitis.
Sources: CODA Collaborative, 2020; Ceresoli, 2019; O’leary, 2021 |
Appendectomy rate
|
No GRADE |
it was not possible to conclude the predefined outcome appendectomy rate in adult patients with acute, uncomplicated appendicitis. Appendectomy rate depends on patient selection for conservative treatment.
Source: Ceresoli, 2019; CODA Collaborative, 2020; Eriksson, 1995; O’Leary, 2021; Salminen, 2015; Salminen, 2018; Sippola, 2020; Styrud, 2006; Vons, 2011. |
Description of studies
De Almeda Leite (2022) conducted a systematic review with meta-analysis of randomized clinical trials evaluating the efficacy of nonoperatieve, antibiotic versus operatieve management of acute uncomplicated appendicitis in adult patients. There were no exclusions based on sex. Non-randomized or quasi-randomized clinical trials, patients presenting with complicated appendicitis (perforation, abscess, or peritonitis), hemodynamically unstable patients (ie, those with shock or septic shock), pediatric patients, and patients with appendicoliths were excluded. The types of interventions compared were conservative (oral, intramuscular, intravenous, or combined antibiotic treatment) versus operative treatment (appendectomy). The trials were conducted between 1995 and 2021, the last search was performed until December 2021.
The seven trials describe 2988 patients which were randomized to conservative treatment (antibiotics, n=1411) or surgical treatment (appendectomy, n=1577). Most studies described a follow-up of one year. For conservative treatment, different types of antibiotics and schedules were precriped, a detailed description is presented in table 1. In addition, different definitions of outcome were used across studies.
Table 1. Desciption of conservative treatment paradigms in De Almeide (2022)
|
Study |
Intravenous antibiotics |
Duration |
Oral antibiotics |
Duration |
|
Eriksson, 1995 |
Cefotaxim 2g two times per day plus tinidazol 800mg once per day |
2 days |
Ofloxacine 200mg plus tinidazol 500mg two times per day |
8 days |
|
Styrud, 2006 |
Cefotaxim 2g two times per day plus tinidazol 800mg per day |
2 days |
Ofloxacine 200mg plus tinidazol 500mg two times per day |
10 days |
|
Vons, 2011 |
Amoxicilline-clavulaanzuur 3–4g per day in patients with nausea or patients who were vomiting |
8-15 days |
Amoxicillin-clavulanate 34g once per day |
8-15 days |
|
Salminen, 2015 |
Ertapenem 1g per day |
3 days |
Levofloxacine 500mg once per day plus metronidazol 500mg three times per day |
7 days |
|
Ceresoli, 2019 |
Ertapenem 1g per day |
3 days |
Amoxicillin- clavulanate 1g 3x per day |
5 days |
|
CODA Collaborative, 2020 |
Formulation (not specified) |
At least 1 day |
Formulation (not specified) |
10 days |
|
O'Leary, 2021
|
Co-amoxiclav, 1.2g three times per day |
Clinical improvement |
Co-amoxiclav 625mg three times per day
|
5 days |
The randomized controlled pilot trial of Talan (2017) investigated the effect of initial antibiotic treatment in comparison with an appendectomy in patients with uncomplicated appendicitis. In total, 30 patients were included and randomly assigned to either antibiotic treatment (n=16) or appendectomy (n=14). Antibiotic treatment contained 300 mg capsules of cefdinir twice daily for adults and children older than thirteen years and seven mg/kg twice daily, maximum 300 mg/dose for children aged five to twelve years. The dose of metronidazole was as follows: for adults and children older than thirteen years, 500-mg tablets three times daily; and for children aged five to twelve years, 10 mg/kg three times daily, maximum 500 mg/dose. The maximum length of follow-up was one year. The reported outcomes in Talan (2017) were complications, appendectomy rate, quality of life, days missed from work due sickness, and length of hospital stay.
The randomized controlled trial of Sippola (2020) aimed to compare antibiotic therapy and appendectomy for treating uncomplicated acute appendicitis. In total, 530 participants, aged between eighteen and 60 years of age, were included and randomized to either antibiotic treatment with intravenous ertapenem (one gram, once daily) for three days followed by seven days of oral levofloxacin (500 milligram, three times per day) or open appendectomy. The CT-criteria for acute appendicitis included an appendiceal diameter exceeding six millimeters with wall thickening accompanied with at least one of the following features: abnormal contrast enhancement of the appediceal wall, inflammatory edema, or fluid collections around the appendix. The maximum length of follow-up was seven years. The reported outcome in Sippola (2020) was the appendectomy rate.
The randomized controlled trial of Salminen (2018) investigated the late recurrence rate of appendicitis after antibiotic therapy for the treatment of uncomplicated acute appendicitis. In total, 530 participants were included and randomly assigned to either antibiotic treatment (n=257) or appendectomy (n=273). Antibiotic treatment consisted of intravenous ertapenem sodium (1 gram per day) for three days, followed by seven days of oral levofloxacin (500 milligram once daily) and metronidazole (500 milligram, three times per day). The maximum length of follow-up was five years. The reported outcomes in Salminen (2018) were the appendectomy rate and complications at five years follow-up.
The inclusion criteria of the RCTs differed on many points. For example, in the Salminen trial, patients with a faecolith were excluded. Only patients with imaging-confirmed uncomplicated appendicitis were included. The CODA trial pragmatically included all patients with acute appendicitis but not by definition uncomplicated appendicitis; CODA only excluded patients with sepsis.
Complications (critical)
Complications within one year follow-up were reported in eight trials (Ceresoli, 2019; CODA Collaborative, 2020; CODA Collaborative, 2021; Eriksson, 1995; Salminen, 2015; Styrud, 2006; Talan, 2017; Vons, 2011). The results were pooled in a meta-analysis (figure 1). The pooled complication rate in the conservative group was 57/1905 (3.0%), compared to 60/1890 (3.2%) in the appendectomy group. This resulted in a pooled relative risk ratio (RR) of 0.94 (95% CI 0.54 to 1.64), in favor of the conservative treatment group. This was considered as a clinically relevant but not statistically significant difference.
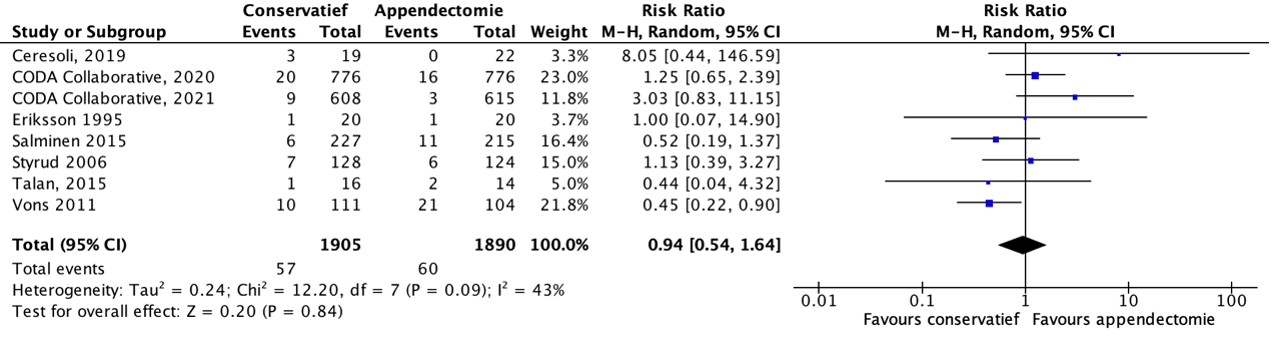
Figure 1. Forest plot showing the comparison between conservative treatment and appendectomy for complications in adult patients with acute, uncomplicated appendicitis. Pooled relative risk ratio, random effects model. Z: p-value of overall effect; df: degrees of freedom; I2; statistical heterogeneity
Ceresoli (2019) reported long-term negative outcomes within one year and defined complications as intervention due to bowel occlusion or intraperitoneal abscess, bowel occlusion longer than 48 hours, incisional hernia or wound dehiscence for the surgical arm.
Complications in the CODA Collaborative (2020) trial in the conservative treatment group were antibiotic reactions (n=1), unplanned admissions to the ICU (n=4), acute renal failures requiring dialysis (n=1), pulmonary embolism requiring therapy (n=1), septic shock requiring pressors (n=1), and hospitalizations other than for treatment of appendicitis (n=19). Complications in the appendectomy group were bleedings (n=1) and hospitalization other than for treatment of appendicitis (n=19).
Salminen (2015) reported the overall complication rate. There were 24 surgical site infections (one organ space, four deep incisional, and nineteen superficial). Four of the five patients in the surgical group with more severe infections had delayed healing of the incision and one patient had persistent incisional pain noted at the two month follow-up.
Styrud (2006) reported complications after surgery, of which most of the complications were wound infections. A specific description of all complications was not reported.
The CODA (2021) trial reported NSQIP-defined complications between 31 days and one year.
Long term complications
Salminen (2018) reported long term complications at five years follow-up and was therefore excluded from the meta-analysis showing complications within one year. The complications rate at five years follow-up in the conservative group was 16/246 (6.5%), compared to 60/246 (24.4%) in the appendectomy group. This resulted in a relative risk ratio (RR) of 0.10 (95% CI 0.04 to 0.23), in favor of the conservative treatment group. In the appendectomy group, two complications were severe requiring a reoperation under general anesthesia (one hernioplasty and one laparoscopic adhesiolysis); all other patients in both study groups had less-severe complications, but were not further specified. This was considered as a clinically relevant difference.
Readmissions (skewed for conservative step-up approach)
Readmission was reported in four trials (Ceresoli, 2019; CODA Collaborative, 2020; Eriksson, 1995; Salminen, 2015). The results were pooled in a meta-analysis. The pooled readmissions rate in the conservative group was 167/1072 (15.6%), compared to 36/1091 (3.3%) in the appendectomy group. This resulted in a pooled relative risk ratio (RR) of 4.58 (95% CI 3.24 to 6.48), a statisitically significant and clinically relevant difference.
However, importantly, in these trials the outcome variable ‘readmissions’ is not a reliable surrogate for complications or a longer recovery in the conservative group, as the trials do not list separate data on readmission for complications versus readmission for delayed appendectomy, the latter applying for the minority of patients as part of the conservative step-up strategy.
Length of hospital stay (important)
Seven included trials in De Almeide Leite (2022) and one additional trial (Talan, 2017) reported the length of hospital stay (in days) at one year follow-up (Ceresoli, 2019; CODA collaborative, 2020; Eriksson, 1995; O’Leary, 2021; Salminen, 2015; Styrud, 2006; Vons, 2011). Most studies reported the mean (SD) length of hospital stay and were pooled in a meta-analysis (figure 3). Talan (2017) reported the median (IQR) length of hospital stay and was therefore reported separately. The pooled mean difference (MD) between the conservative group (n=1411) and appendectomy group (n=1423) for length of hospital stay was 0.18 days (95% CI -0.09 to 0.46), no clinically relevant difference, with a shorter length of hospital stay in days in the appendectomy group.
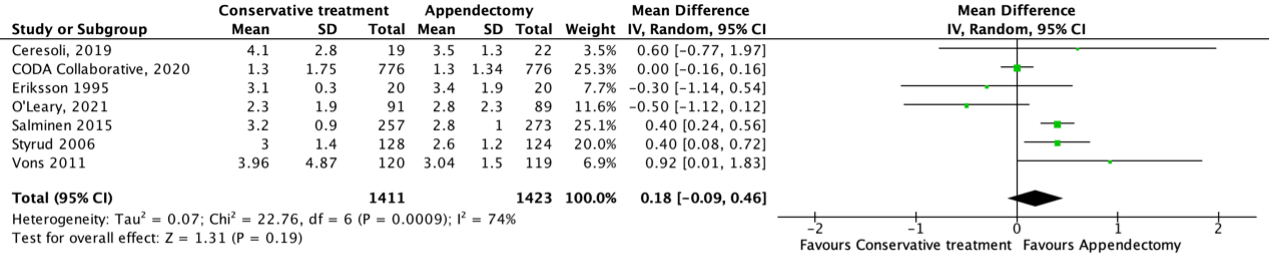
Figure 2. Forest plot showing the comparison between conservative treatment and appendectomy for the length of hospital stay in adult patients with acute, uncomplicated appendicitis. Pooled mean difference, random effects model. Z: p-value of overall effect; df: degrees of freedom; I2; statistical heterogeneity
Talan (2017) reported the total median (IQR) time in the hospital in hours. The median (IQR) length of hospital stay in the conservative group (n=16) was 16.2 (14.2 to 34.3) hours, compared to 42.1 (28.8 to 65.0) hours in the appendectomy group (n=14). This was considered as a clinically relevant difference.
Salminen (2018) also reported the length of hospital stay (both primary hospitalization and all additional hospital stays) at three, five, and ten years follow-up, but reported the median (95% CI) length of hospital stay. The median (IQR) length of hospital stay in the appendectomy group was 3 (95% CI 3 to 3) days, compared to 3 (95% CI 3 to 3) days in the conservative group. This was not considered as a clinically relevant difference.
Quality of life (important)
Quality of life was determined by the EQ-5D and reported in two trials (CODA Collaborative, 2020; O’Leary, 2021) and in one additional trial (Talan, 2017). The results of the CODA Collaborative (2020) and O’Leary (2021) were pooled in a meta-analysis (figure 4). Talan (2017) reported the median (IQR) SF-12 score and was reported separately. The mean difference (MD) between the conservative group (n=861) and the appendectomy group (n=865) was -0.00 (95% CI -0.04 to 0.03), no clinically relevant difference in quality of life between groups.

Figure 3. Forest plot showing the comparison between conservative treatment and appendectomy for quality of life in adult patients with acute, uncomplicated appendicitis. Pooled std. mean difference, random effects model. Z: p-value of overall effect; df: degrees of freedom; I2; statistical heterogeneity
The median (IQR) SF-12 score in Talan (2017) for the physical component at one month follow-up in the conservative group was 54 (52 to 58) points, compared to 44 (36 to 51) points in the appendectomy group. This was considered as a clinically relevant difference.
The median (IQR) SF-12 score in Talan (2017) for the mental component at one month follow-up in the conservative group was 55 (49 to 57) points, compared to 56 (43 to 58) points in the appendectomy group. This was considered as a clinically relevant difference.
Days missed from work due to sickness (important)
In total, three studies reported the number of days missed from work due to sickness (CODA Collaborative, 2020; O’Leary, 2021; Salminen, 2015). Due to the heterogeneity in reported outcome and statistics, it was not possible to pool the data. Therefore, we describe the results from the different studies separately.
The CODA Collaborative (2020) reported on the total number of days missed from work within 90 days. The mean (SD) number of days missed work in the conservative group (n=478) was 5.26 (23.2862) days versus 8.73 days (23.2862) in the surgical group (n=473). The authors computed the data and calculated a mean difference (MD) of -3.47 (95%CI -6.43 to -0.51), a clinically relevant difference favoring the conservative group.
Ceresoli (2019) analyzed the total number of sick leave days. The mean (SD) number of sick leave days was 8.5 (7.9) in the conservative group (n=19) versus 11.4 (5.3) in the surgical group (n=22). This resulted in a mean difference (MD) of -2.90 (95%CI -7.09 to 1.29) days, no clinically relevant difference between the groups.
O’leary (2021) analyzed the accumulated 12-month sickness days. The mean (SD) 12-month sickness days was 0.5 (1.9207) days in the conservative group (n=91) versus 0.05 (0.2374) days in the surgical group. Resulting in a mean difference (MD) of 0.45 days (95% CI 0.05 to 0.85), no clinically relevant difference between the groups.
Appendectomy rate
Appendectomy rates were reported in all seven trials (Ceresoli, 2019; CODA Collaborative, 2020; Eriksson, 1995; O’Leary, 2021; Salminen, 2015; Styrud, 2006; Vons, 2011). The outcome of the number of appendectomies corresponds to the control intervention of this guideline and therefore, the number of appendectomies in the control group automatically reaches 100%. Therefore, the number of patients who underwent an appendectomy within one year follow-up after initial conservative treatment are reported descriptively. If available, we also presented the long term follow-up results for the number of patients who needed appendectomy after initial conservative treatment (table 2).
Table 2: Appendectomy rate within 90 days, one year, one and five years and more than five years after initial conservative treatment of acute, uncomplicated appendicitis
|
Author (year of publication) |
Appendectomy rate within 90 days after initial conservative treatment |
|
CODA Collaborative (2020) |
212/776 (27.3%) |
|
Talan (2017)
|
0/16 (0%) |
|
Author (year of publication) |
Appendectomy rate within one year after initial conservative treatment |
|
Ceresoli (2019) |
3/19 (15.8%) |
|
CODA Collaborative (2021) |
40.0% (exact numbers not reported) |
|
Eriksson (1995) |
7/20 (35.0%) |
|
O’Leary (2021) |
23/91 (25.3%) |
|
Salminen (2015) |
70/256 (27.3%) |
|
Styrud (2006) |
16/128 (12.5%) |
|
Vons (2011) |
44/120 (36.7%)
|
|
Author (year of publication) |
Appendectomy rate between up to five years after initial conservative treatment |
|
Salminen (2018) Two years Three years Four years Five years
|
87/256 (34%) 90/256 (35.2%) 95/256 (37.1%) 100/256 (39.1%) |
|
CODA Collaborative (2021) Two years Three years Four years |
46.0% (exact numbers not reported) 49.0% (exact number not reported) 49.0% (exact numbers not reported)
|
|
Author (year of publication) |
Appendectomy rate after five years follow-up after initial conservative treatment |
|
Sippola (2020) |
81/206 (39.3%) |
Level of evidence of the literature
Complications (critical)
The level of evidence regarding the outcome complications was derived from randomized controlled trials and therefore started high. The level of evidence was downgraded by two levels because of the wide confidence interval crossing both boundaries of clinical relevance (imprecision, -2). The level of evidence was considered as low.
Readmissions (important)
The level of evidence regarding the outcome readmission was derived from randomized controlled trials and therefore started high. The level of evidence was downgraded by one level because of the small number of events (imprecision, -1). The level of evidence was considered as moderate.
Length of hospital stay (important)
The level of evidence regarding the outcome length of hospital stay was derived from randomized controlled trials and therefore started high. The level of evidence was downgraded by two levels because of the small number of events, and the wide confidence interval crossing the lower and upper boundaries of clinical relevance (imprecision, -2). The level of evidence was considered as low.
Quality of life (important)
The level of evidence regarding the quality of life was derived from randomized controlled trials and therefore started high. The level of evidence was downgraded by three levels because of a lack of blinding (risk of bias, -1), the small number of participants (imprecision, -2). The level of evidence was considered as very low.
Days missed from work due to sickness (important)
The level of evidence regarding the outcome days missed from work due to sickness was derived from randomized controlled trials and therefore started high. The level of evidence was downgraded by three levels because of the heterogeneity in reported outcomes (-1), which resulted in low statistical power due to individual study analyses (-1), and the wide confidence intervals (imprecision, -1). The level of evidence was considered as very low.
Appendectomy rate
Due to the fact that the outcome is similar to the control intervention and could only be represented descriptively, it was not possible to grade the literature for the appendectomy rate between conservative treatment and treatment with appendectomy in patients with acute, uncomplicated appendicitis.
A systematic review of the literature was performed to answer the following question:
What are the (un)beneficial effects of conservative treatment using intravenous antibiotics in comparison with appendectomy in adult patients with acute, uncomplicated appendicitis?
PICO 1
P: Adult patients with acute, uncomplicated appendicitis.
I: Conservative treatment using (intravenous) antibiotics.
C: Appendectomy.
O: Appendectomy rate, complications, readmissions, length of hospital stay, quality of life, and days missed from work due to sickness.
Relevant outcome measures
The guideline development group considered complications as a critical outcome measure for decision making; recurrence, readmissions, length of hospital stay, quality of life, days missed from work due to sickness, and the appendectomy rate (short and long term) were considered as important outcome measures.
The guideline development group defined a relative risk (RR) for dichotomous outcomes of <0.80 and >1.25 as a minimal clinically (patient) important difference, this applies to both predefined outcomes.
Search and select (Methods)
The databases Medline (via OVID) and Embase (via Embase.com) were searched with relevant search terms until the 22th of August 2022. The detailed search strategy is depicted under the tab Methods. The systematic literature search resulted in 440 hits. Studies were selected based on the following criteria: systematic reviews and randomized controlled trials (RCTs) describing the effect of conservative treatment, using antibiotics versus appendectomy in adult patients aged 18 years and older presenting with acute uncomplicated appendicitis. Thirty-six studies were initially selected based on title and abstract screening. After reading the full texts, 33 were excluded (see the table with reasons for exclusion under the tab Methods).
Results
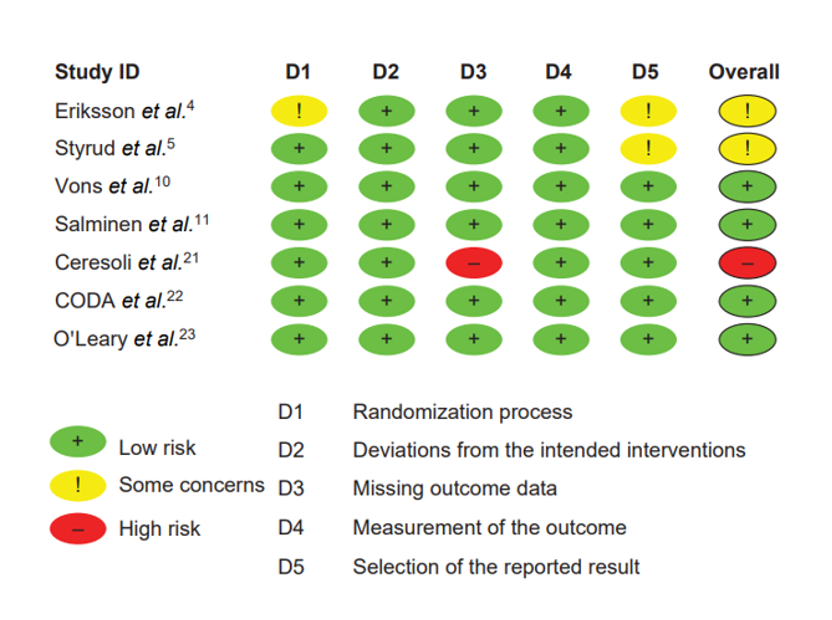
One systematic review including eight relevant RCTs and two individual RCTs were included in the analysis of the literature. From the eight studies in the systematic review, one study was additionally excluded for the purpose of this guideline as Hansson (2009) described a quasi-randomized trial. Important study characteristics and results are summarized in the evidence tables. The assessment of the risk of bias is summarized in the risk of bias tables.
- Bhangu A, Søreide K, Di Saverio S, Assarsson JH, Drake FT. Acute appendicitis: modern understanding of pathogenesis, diagnosis, and management. Lancet. 2015 Sep 26;386(10000):1278-1287. doi: 10.1016/S0140-6736(15)00275-5. Erratum in: Lancet. 2017 Oct 14;390(10104):1736. PMID: 26460662.
- Ceresoli M, Pisano M, Allievi N, Poiasina E, Coccolini F, Montori G, Fugazzola P, Ansaloni L. Never put equipoise in appendix! Final results of ASAA (antibiotics vs. surgery for uncomplicated acute appendicitis in adults) randomized controlled trial. Updates Surg. 2019 Jun;71(2):381-387. doi: 10.1007/s13304-018-00614-z. Epub 2018 Dec 17. PMID: 30560527.
- CODA Collaborative; Flum DR, Davidson GH, Monsell SE, Shapiro NI, Odom SR, Sanchez SE, Drake FT, Fischkoff K, Johnson J, Patton JH, Evans H, Cuschieri J, Sabbatini AK, Faine BA, Skeete DA, Liang MK, Sohn V, McGrane K, Kutcher ME, Chung B, Carter DW, Ayoung-Chee P, Chiang W, Rushing A, Steinberg S, Foster CS, Schaetzel SM, Price TP, Mandell KA, Ferrigno L, Salzberg M, DeUgarte DA, Kaji AH, Moran GJ, Saltzman D, Alam HB, Park PK, Kao LS, Thompson CM, Self WH, Yu JT, Wiebusch A, Winchell RJ, Clark S, Krishnadasan A, Fannon E, Lavallee DC, Comstock BA, Bizzell B, Heagerty PJ, Kessler LG, Talan DA. A Randomized Trial Comparing Antibiotics with Appendectomy for Appendicitis. N Engl J Med. 2020 Nov 12;383(20):1907-1919. doi: 10.1056/NEJMoa2014320. Epub 2020 Oct 5. PMID: 33017106.
- CODA Collaborative. (2021). Antibiotics versus appendectomy for acute appendicitis—longer-term outcomes. New England Journal of Medicine, 385(25), 2395-2397.
- de Almeida Leite RM, Seo DJ, Gomez-Eslava B, Hossain S, Lesegretain A, de Souza AV, Bay CP, Zilberstein B, Marchi E, Machado RB, Barchi LC, Ricciardi R. Nonoperative vs Operative Management of Uncomplicated Acute Appendicitis: A Systematic Review and Meta-analysis. JAMA Surg. 2022 Sep 1;157(9):828-834. doi: 10.1001/jamasurg.2022.2937. PMID: 35895073; PMCID: PMC9330355.
- Margenthaler, J.A., et al., Risk factors for adverse outcomes after the surgical treatment of appendicitis in adults. Ann Surg, 2003. 238(1): p. 59-66.
- Livingston, E.H., et al., Epidemiological similarities between appendicitis and diverticulitis suggesting a common underlying pathogenesis. Arch Surg, 2011. 146(3): p. 308-14.
- O'Leary DP, Walsh SM, Bolger J, Baban C, Humphreys H, O'Grady S, Hegarty A, Lee AM, Sheehan M, Alderson J, Dunne R, Morrin MM, Lee MJ, Power C, McNamara D, McCawley N, Robb W, Burke J, Sorensen J, Hill AD. A Randomized Clinical Trial Evaluating the Efficacy and Quality of Life of Antibiotic-only Treatment of Acute Uncomplicated Appendicitis: Results of the COMMA Trial. Ann Surg. 2021 Aug 1;274(2):240-247. doi: 10.1097/SLA.0000000000004785. PMID: 33534226.
- Salminen P, Paajanen H, Rautio T, Nordström P, Aarnio M, Rantanen T, Tuominen R, Hurme S, Virtanen J, Mecklin JP, Sand J, Jartti A, Rinta-Kiikka I, Grönroos JM. Antibiotic Therapy vs Appendectomy for Treatment of Uncomplicated Acute Appendicitis: The APPAC Randomized Clinical Trial. JAMA. 2015 Jun 16;313(23):2340-8. doi: 10.1001/jama.2015.6154. PMID: 26080338.
- Talan DA, Saltzman DJ, Mower WR, Krishnadasan A, Jude CM, Amii R, DeUgarte DA, Wu JX, Pathmarajah K, Morim A, Moran GJ; Olive View–UCLA Appendicitis Study Group. Antibiotics-First Versus Surgery for Appendicitis: A US Pilot Randomized Controlled Trial Allowing Outpatient Antibiotic Management. Ann Emerg Med. 2017 Jul;70(1):1-11.e9. doi: 10.1016/j.annemergmed.2016.08.446. Epub 2016 Dec 11. PMID: 27974169; PMCID: PMC5616169.
- Vons C, Barry C, Maitre S, Pautrat K, Leconte M, Costaglioli B, Karoui M, Alves A, Dousset B, Valleur P, Falissard B, Franco D. Amoxicillin plus clavulanic acid versus appendicectomy for treatment of acute uncomplicated appendicitis: an open-label, non-inferiority, randomised controlled trial. Lancet. 2011 May 7;377(9777):1573-9. doi: 10.1016/S0140-6736(11)60410-8. PubMed PMID: 21550483.
- Salminen P, Tuominen R, Paajanen H, Rautio T, Nordström P, Aarnio M, Rantanen T, Hurme S, Mecklin JP, Sand J, Virtanen J, Jartti A, Grönroos JM. Five-Year Follow-up of Antibiotic Therapy for Uncomplicated Acute Appendicitis in the APPAC Randomized Clinical Trial. JAMA. 2018 Sep 25;320(12):1259-1265. doi: 10.1001/jama.2018.13201. PubMed PMID: 30264120. COLLINS DC. 71,000 HUMAN APPENDIX SPECIMENS. A FINAL REPORT, SUMMARIZING FORTY YEARS' STUDY. Am J Proctol. 1963 Dec;14:265-81. PubMed PMID: 14098730.
- Sammalkorpi, H.E., P. Mentula, and A. Leppaniemi, A new adult appendicitis score improves diagnostic accuracy of acute appendicitis--a prospective study. BMC Gastroenterol, 2014. 14: p. 114.
- Sippola S, Grönroos J, Tuominen R, Paajanen H, Rautio T, Nordström P, Aarnio M, Rantanen T, Hurme S, Salminen P. Economic evaluation of antibiotic therapy versus appendicectomy for the treatment of uncomplicated acute appendicitis from the APPAC randomized clinical trial. Br J Surg. 2017 Sep;104(10):1355-1361. doi: 10.1002/bjs.10575. Epub 2017 Jul 5. PubMed PMID: 28677879.
- Sippola S, Haijanen J, Viinikainen L, Grönroos J, Paajanen H, Rautio T, Nordström P, Aarnio M, Rantanen T, Hurme S, Mecklin JP, Sand J, Jartti A, Salminen P. Quality of Life and Patient Satisfaction at 7-Year Follow-up of Antibiotic Therapy vs Appendectomy for Uncomplicated Acute Appendicitis: A Secondary Analysis of a Randomized Clinical Trial. JAMA Surg. 2020 Apr 1;155(4):283-289. doi: 10.1001/jamasurg.2019.6028. PMID: 32074268; PMCID: PMC7042917.
- Styrud J, Eriksson S, Nilsson I, Ahlberg G, Haapaniemi S, Neovius G, Rex L, Badume I, Granström L. Appendectomy versus antibiotic treatment in acute appendicitis. a prospective multicenter randomized controlled trial. World J Surg. 2006 Jun;30(6):1033-7. doi: 10.1007/s00268-005-0304-6. PMID: 16736333.
- Wagner, M., D.J. Tubre, and J.A. Asensio, Evolution and Current Trends in the Management of Acute Appendicitis. Surg Clin North Am, 2018. 98(5): p. 1005-1023.
|
Study reference |
Study characteristics |
Patient characteristics 2 |
Intervention (I) |
Comparison / control (C) 3
|
Follow-up |
Outcome measures and effect size 4 |
Comments |
|
Ceresoli (2019) |
Type of study: RCT.
Funding and conflicts of interest: All authors declare that they have no confict of interest.
|
Inclusion criteria:
Exclusion criteria:
N total at baseline: Conservative: N = 19 Appendectomy: N = 22
|
Describe intervention (treatment/procedure/test):
Conservative treatment
|
Describe control (treatment/procedure/test):
Appendectomy |
Length of follow-up: 1 year.
Loss-to-follow-up: None.
|
Appendectomy rate I: 3/19 (15.8%)* C: 22/22 (100%)
*1 patient worsened between the 1st and second ertapenem administration and was operated with no complications. One worsened between the 2nd and 3rd administration and at operation was found to have complicated appendicitis (perforation), while the 3rd patient worsened after the third dose of antibiotic.
Long-term negative outcomes within a year (re-intervention due to bowel occlusion or intraperitoneal abscess, bowel occlusion longer than 48 hours, intraperitoneal abscess, incisional hernia or wound dehiscence for surgical arm; recurrence of AA in the antibiotic arm). I: 1/16 (6.2%)** C: 5/22 (22.7%)
**1 patient experienced relapse of acute appendicitis at 30 days from the third dose of ertapenem: according to the protocol, he underwent surgery and an uneventful laparoscopic appendectomy was performed; no complications were observed. No further events or complications were observed at 1-year follow-up.
Length of hospital stay, mean (SD) I: 4.1 (2.8) C: 3.5 (1.3)
Length of work absence I: 8.5 (7.9) C: 11.4 (5.3) |
Author’s conclusion: In conclusion, the dogmatic indication to surgery in case of suspected acute appendicitis allowed saving many lives in pre-antibiotic era. However, this approach has decreased the stimulus to investigate the role of the vermiform appendix, to understand the primium movens of acute inflammation of the appendix, to reach a broad agreement on the diagnosis and on the diagnostic tools, to establish a common histopathological classification and to find a worldwide accepted definition of uncomplicated and complicated acute appendicitis. Unfortunately, the present study does not add further evidences on this intricated topic; however, it demonstrates the great difficulty in providing evidence-based answers to questions directly arising from daily surgical practice. |
|
CODA collaborative (2020) |
Type of study: RCT.
Funding and conflicts of interest: The CODA trial was funded by the Patient-Centered Outcomes Research Institute.
The CODA Collaborative writing committee assumes responsibility for the content of this article. The views presented in this work are solely the responsibility of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute, its board of governors, or its methodology committee. Supported by a Patient-Centered Outcomes Research Institute Award (1409-240099). Dr. Evans reports receiving advisory board fees from Tetraphase Pharmaceuticals; Dr. Moran, receiving grant support from Allergan, ContraFect, and Nabriva; Dr. Park, receiving grant support from Bristol Myers Squibb and Atox Bio; and Dr. Winchell, receiving consulting fees from Stryker. No other potential conflict of interest relevant to this article was reported.
|
Inclusion criteria:
Exclusion criteria:
N total at baseline: Conservative: N = 776 Appendectomy: N = 776
|
Describe intervention (treatment/procedure/test):
Conservative treatment.
|
Describe control (treatment/procedure/test):
Appendectomy. |
Length of follow-up: 90 days.
Loss-to-follow-up: I: N = 96 C: N = 114
|
Appendectomy rate 90 days FU I: 196/676 (29.0%) C: 656/656 (100%)
EQ-5D score I: 0.92 (0.13) C: 0.91 (0.13)
Complications* I: 27/676 (4.0%) C: 20/656 (3.0%)
*Complications antibiotic group: - 1 severe antibiotic reaction - 4 unplanned admits to ICU - 1 acute renal failure requiring dialysis - 1 pulmonary embolism requiring therapy - 1 septic shock requiring pressors - 19 hospitalizations other than for treatment of appendicitis.
Complications surgery group: - 1 bleeding requiring transfusion - 19 hospitalization other than for treatment of appendicitis.
Days in hospital after index treatment, number of days/number of participants (mean) I: 421/622 (0.68) C: 93/609 (0.15)
Long term results at 2 and 3 years follow-up. The CODA Collaborative (2020) also reported the number of patients who underwent an appendectomy within two and three years after initial conservative treatment. The appendectomy rate within two years after initial conservative treatment of acute, uncomplicated appendicitis was 41/62 (66.1%). The appendectomy rate within three years of initial conservative treatment of acute, uncomplicated appendicitis was 5/9 (55.5%). |
Author’s conclusion:
|
|
Eriksson (1995) |
Type of study: RCT.
Funding and conflicts of interest: The authors thank Dr Gunnar Granstrom, Department of Infectious Diseases, Karolinska Institute, Danderyd Hospital, for help in designing the antibiotic treatment and Dr Anders Moberg, Depanment of Pathology, Danderyd Hospital, for pathological evaluation. This work was supported by the Danderyd Hospital, the funds of the Karolinska Institute, Swedish Hoechst AB, Pfizer AB and the Mutual Group Life Insurance Company 'Forenade Liv', Stockholm, Sweden. |
Inclusion criteria:
Exclusion criteria:
N total at baseline: Intervention: N = 20 Control: N = 20
|
Describe intervention (treatment/procedure/test):
Conservative treatment.
|
Describe control (treatment/procedure/test):
Appendectomy |
Length of follow-up: 30 days.
Loss-to-follow-up: None.
|
Appendectomy rate* I: 7/20 (35%) C: 20/20 (100%)
*Seven patients given antibiotic treatment were readmitted with recurrent appendicitis (six had phlegmonous appendicitis and one a perforated appendicitis after 15h of pain before hospitalization). Surgery occurred after a mean of 7 (range 3 to 12) months after conservative treatment. |
Author’s conclusion: The study indicates patients' interest in conservative treatment as 40 of 45 agreed to participate in the study despite being informed about the risk for recurrence. |
|
O’Leary (2021) |
Type of study: RCT.
Funding and conflicts of interest: The authors report no conflicts of interest.
|
Inclusion criteria:
Exclusion criteria:
N total at baseline: Intervention: N = 91 Control: N = 89
|
Describe intervention (treatment/procedure/test):
Conservative treatment
|
Describe control (treatment/procedure/test):
Appendectomy |
Length of follow-up: 12 months.
Loss-to-follow-up: None.
|
Appendectomy rate within 1 year FU I: 23/91 (25.3%) C: 89/89 (100%)
Appendectomy rate later than 1 year FU I: 29*/91 (31.9%) C: 89/89 (100%)
*Additional 6 patients to the 23 patients with an required appendectomy within 1 year follow-up.
EQ-5D, mean (95% CI) I: 0.439 (95% CI 0.319 to 0.560) C: 0,876 (95% CI 0,808 to 0.945
Pain, mean (95% CI) (0-10) I: 0.3 (95% CI 0.1 to 0.5) C: 0.1 (95% CI 0.0 to 0.2)
Sickness days I: 5.3 days C: 8.9 days
Length of stay I: 2.8 days C: 2.3 days |
Author’s conclusion: Patients with acute, uncomplicated appendicitis treated with antibiotics only endure high recurrence rates and an inferior quality of life, when assessed prospectively. Surgery should remain the mainstay of treatment for this commonly encountered acute surgical condition. |
|
Salminen (2015) |
Type of study: RCT.
Funding and conflicts of interest: The authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Salminen reported receiving personal fees for lectures from Merck and Roche. No other disclosures were reported.
The APPAC trial was supported by a government research grant (EVO Foundation) awarded to Turku University Hospital.
|
Inclusion criteria:
Exclusion criteria:
N total at baseline: Intervention: N = 257 Control: N = 273
|
Describe intervention (treatment/procedure/test):
Conservative treatment |
Describe control (treatment/procedure/test):
Appendectomy. |
Length of follow-up: 1 year.
Loss-to-follow-up: I: N = 29 C: N = 57
|
Appendectomy rate I: 70/256 (27.3%) C: 272/273 (99.6%)
Complications* I: 6/216 (2.8%) (95% CI 1.0 to 6.0) C: 45/220 (20.5%) (95% 15.3 to 26.4)
*Overall complications, not specified.
Length of hospital stay (primary hospitalization), median (IQR) I: 3 (3 to 3) days. C: 3 (2 to 3) days.
Pain at discharge, median (IQR) I: 2.0 (1 to 2) C: 3.0 (2 to 4)
Pain at 1 week FU, median (IQR) I: 1.0 (1 to 1) C: 2.0 (1 to 3)
Pain at 2 months FU, median (IQR) I: 1.0 (1 to 1) C: 1.0 (1 to 1)
Length of sick leave, median (IQR) I: 7.0 (7 to 12) days. C: 19.0 (14 to 21) days. |
Author’s conclusion: Among patients with CT-proven, uncomplicated appendicitis, antibiotic treatment did not meet the prespecified criterion for noninferiority compared with appendectomy.Most patients randomized to antibiotic treatment for uncomplicated appendicitis did not require appendectomy during the 1-year follow-up period, and those who required appendectomy did not experience significant complications. |
|
Salminen (2018)
|
Type of study: RCT.
Funding: This trial was supported by the Mary and Georg C. Ehrnrooth Foundation, a government research grant (EVO Foundation) awarded to Turku University Hospital, and a Turku University research grant.
None of the funding entities had a role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Conflict of interest disclosures: All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Salminen reports receipt of personal fees for lectures from Merck, Lilly, and Orion Pharma. No other disclosures were reported. |
Inclusion criteria:
Exclusion criteria:
N total at baseline: Intervention: N = 257 Control: N = 273
|
Describe intervention (treatment/procedure/test):
Conservative treatment |
Describe control (treatment/procedure/test):
Appendectomy. |
Length of follow-up: 7 years.
Loss-to-follow-up: I: N = 30 C: N = 58
|
Appendectomy rate between one and five years after initial conservative treatment I: 30/81 (37.0%) C: 273/273 (100%)
|
Author’s conclusion Among patients who were initially treated with antibiotics for uncomplicated acute appendicitis, the likelihood of late re- currence within 5 years was 39.1%. This long-term follow-up supports the feasibility of antibiotic treatment alone as an al- ternative to surgery for uncomplicated acute appendicitis. |
|
Sippola (2020) |
Type of study: RCT.
Funding: This trial was supported by the Mary and Georg C. Ehrnrooth Foundation and a government research grant awarded to Turku University Hospital.
The funding organizations had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Conflict of interest disclosures: Dr Sippola reported grants from Mary and Georg C. Ehrnrooth Foundation and Turku University Hospital during the conduct of the study. Dr Salminen reported personal fees from Orion Pharma and Merck outside the submitted work. No other disclosures were reported. |
Inclusion criteria:
Exclusion criteria:
N total at baseline: Intervention: N = 257 Control: N = 273
|
Describe intervention (treatment/procedure/test):
Conservative treatment |
Describe control (treatment/procedure/test):
Appendectomy. |
Length of follow-up: 7 years.
Loss-to-follow-up: I: N = 15 C: N = 1
|
Appendectomy rate I: 70/81 (86.4%) C: 273/273 (100%)
|
Author’s conclusion Long-term QOL is similar after appendectomy and antibiotic therapy for treating uncomplicated acute appendicitis. Pa- tients taking antibiotics who later underwent appendectomy were less satisfied than patients with successful antibiotic treatment or appendectomy, underlining the importance of discovering potential parameters predictive of appendicitis recurrence. |
|
Styrud (2006) |
Type of study: RCT.
Funding and conflicts of interest: This work was supported by research funds of the Swedish Society of Medicine, Karolinska Institutet; the Wallenius Corporation; Aventis Pharma (former Hoecht Marion Roussel). We are indebted to G. Orrebrink and O. Sta˚hlebrandt for their contributions to this study.
|
Inclusion criteria:
Exclusion criteria:
N total at baseline: Intervention: N = 124 Control: N = 128
|
Describe intervention (treatment/procedure/test):
Conservative treatment.
|
Describe control (treatment/procedure/test):
Appendectomy. |
Length of follow-up: 1 year.
Loss-to-follow-up: None.
|
Appendectomy rate I: 16/128 (12.5%) C: 124/124 (100%)
Complications I: 4/128 (3.1%) C: 17**/124 (17%)
*Complications after surgery. **Mainly wound infections.
Length of hospital stay I: 3.0 (1.4) days. C: 2.6 (1.2) days.
Days of sick leave I: 5.3 (4.1) C: 6.0 (4.4)
Time off work C: 10.1 (7.6) |
Author’s conclusion: In conclusion, this study shows that acute appendicitis can be treated successfully with antibiotics with a short hospital stay, minimal sick leave, and limited duration of pain. There is a risk of recurrence, which should be compared with the rate of complications after appendectomy. |
|
Vons (2011) |
Type of study: RCT.
Funding and conflicts of interest: The sponsor of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report. CV, CB, BF, and DF had full access to all data in the study and fi nal responsibility for the decision to submit for publication. All other authors could request examination of any of the data elements.
Funding French Ministry of Health, Programme Hospitalier de Recherche Clinique 2002.
We declare that we have no confl icts of interest.
|
Inclusion criteria:
Exclusion criteria:
N total at baseline: Intervention: N = 120 Control: N = 119 |
Describe intervention (treatment/procedure/test):
Conservative treatment.
|
Describe control (treatment/procedure/test):
Appendectomy. |
Length of follow-up: 1 year.
Loss-to-follow-up:
|
Appendectomy rate I: 39/120 (32.5%) C: 119/119 (100%)
|
Author’s conclusion:
|
Quality assessment
Algemene informatie
|
Cluster/richtlijn: GE-chirurgie; acute appendicitis |
|
|
Uitgangsvraag/modules: Welke behandeling heeft de voorkeur bij volwassen patiënten met een acute simpele appendicitis? |
|
|
Database(s): Ovid/Medline, Embase.com |
Datum: 22 augustus 2022 |
|
Periode: 2000 - heden |
Talen: Engels, Nederlands |
|
Literatuurspecialist: Miriam van der Maten |
|
|
BMI-zoekblokken: voor verschillende opdrachten wordt (deels) gebruik gemaakt van de zoekblokken van BMI-Online https://blocks.bmi-online.nl/ Bij gebruikmaking van een volledig zoekblok zal naar de betreffende link op de website worden verwezen. |
|
|
Toelichting: Voor deze vraag is gezocht op de elementen:
Het sleutelartikel van Bom (Population preference for treatment of uncomplicated appendicitis) wordt niet gevonden met de search omdat het niet geïndexeerd is als RCT of SR. Qua zoektermen zou het wel uit de search komen. |
|
|
Te gebruiken voor richtlijnen tekst: Nederlands In de databases Embase.com en Ovid/Medline is op 22 augustus 2022 met relevante zoektermen gezocht naar systematische reviews en RCT over de behandelingsvoorkeur bij volwassenen met acute appendicitis. De literatuurzoekactie leverde 440 unieke treffers op.
Engels On the 22nd of August, relevant search terms were used to search for systematic reviews and RCT about the preferred treatment for adults with acute appendicitis in the databases Embase.com and Ovid/Medline. The search resulted in 440 unique hits. |
|
Zoekopbrengst
|
|
EMBASE |
OVID/MEDLINE |
Ontdubbeld |
|
SRs |
169 |
166 |
191 |
|
RCT |
199 |
223 |
249 |
|
Totaal |
368 |
389 |
440 |
Zoekstrategie
Embase.com
|
No. |
Query |
Results |
|
#17 |
#15 OR #16 |
368 |
|
#16 |
#12 AND #14 NOT #15 = RCT |
199 |
|
#15 |
#12 AND #13 = SR |
169 |
|
#14 |
'randomized controlled trial'/exp OR random*:ti,ab OR (((pragmatic OR practical) NEAR/1 'clinical trial*'):ti,ab) OR ((('non inferiority' OR noninferiority OR superiority OR equivalence) NEAR/3 trial*):ti,ab) OR rct:ti,ab,kw |
1947413 |
|
#13 |
'meta analysis'/exp OR 'meta analysis (topic)'/exp OR metaanaly*:ti,ab OR 'meta analy*':ti,ab OR metanaly*:ti,ab OR 'systematic review'/de OR 'cochrane database of systematic reviews'/jt OR prisma:ti,ab OR prospero:ti,ab OR (((systemati* OR scoping OR umbrella OR 'structured literature') NEAR/3 (review* OR overview*)):ti,ab) OR ((systemic* NEAR/1 review*):ti,ab) OR (((systemati* OR literature OR database* OR 'data base*') NEAR/10 search*):ti,ab) OR (((structured OR comprehensive* OR systemic*) NEAR/3 search*):ti,ab) OR (((literature NEAR/3 review*):ti,ab) AND (search*:ti,ab OR database*:ti,ab OR 'data base*':ti,ab)) OR (('data extraction':ti,ab OR 'data source*':ti,ab) AND 'study selection':ti,ab) OR ('search strategy':ti,ab AND 'selection criteria':ti,ab) OR ('data source*':ti,ab AND 'data synthesis':ti,ab) OR medline:ab OR pubmed:ab OR embase:ab OR cochrane:ab OR (((critical OR rapid) NEAR/2 (review* OR overview* OR synthes*)):ti) OR ((((critical* OR rapid*) NEAR/3 (review* OR overview* OR synthes*)):ab) AND (search*:ab OR database*:ab OR 'data base*':ab)) OR metasynthes*:ti,ab OR 'meta synthes*':ti,ab |
733409 |
|
#12 |
#9 AND #10 AND #11 AND ([english]/lim OR [dutch]/lim) AND [2000-2022]/py NOT ('conference abstract'/it OR 'editorial'/it OR 'letter'/it OR 'note'/it) NOT (('animal experiment'/exp OR 'animal model'/exp OR 'nonhuman'/exp) NOT 'human'/exp) |
1921 |
|
#11 |
'appendectomy'/exp/mj OR 'laparoscopy'/exp/mj OR appendectom*:ti,ab,kw OR 'surgery'/exp/mj OR 'surgery'/lnk OR surgical:ti,ab,kw OR surger*:ti,ab,kw OR operation*:ti,ab,kw OR operative:ti,ab,kw |
5876084 |
|
#10 |
'conservative treatment'/exp/mj OR conservative:ti,ab,kw OR noninvasive:ti,ab,kw OR 'non invasive':ti,ab,kw OR nonsurg*:ti,ab,kw OR 'non surg*':ti,ab,kw OR nonoperati*:ti,ab,kw OR 'non operati*':ti,ab,kw OR 'drug therapy'/exp/mj OR 'intravenous drug administration'/exp/mj OR intravenous:ti,ab,kw OR ((drug NEAR/2 (treat* OR therap*)):ti,ab,kw) OR 'antiinfective agent'/exp/mj OR antibacterial*:ti,ab,kw OR ((anti NEAR/1 bacterial*):ti,ab,kw) OR antibiotic*:ti,ab,kw |
4063348 |
|
#9 |
'appendicitis'/exp/mj OR appendicit*:ti,ab,kw |
30103 |
Ovid/Medline
|
# |
Searches |
Results |
|
11 |
9 or 10 |
389 |
|
10 |
(6 and 8) not 9 = RCT |
223 |
|
9 |
6 and 7 = SR |
166 |
|
8 |
exp randomized controlled trial/ or randomized controlled trials as topic/ or random*.ti,ab. or rct?.ti,ab. or ((pragmatic or practical) adj "clinical trial*").ti,ab,kf. or ((non-inferiority or noninferiority or superiority or equivalence) adj3 trial*).ti,ab,kf. |
1538779 |
|
7 |
meta-analysis/ or meta-analysis as topic/ or (metaanaly* or meta-analy* or metanaly*).ti,ab,kf. or systematic review/ or cochrane.jw. or (prisma or prospero).ti,ab,kf. or ((systemati* or scoping or umbrella or "structured literature") adj3 (review* or overview*)).ti,ab,kf. or (systemic* adj1 review*).ti,ab,kf. or ((systemati* or literature or database* or data-base*) adj10 search*).ti,ab,kf. or ((structured or comprehensive* or systemic*) adj3 search*).ti,ab,kf. or ((literature adj3 review*) and (search* or database* or data-base*)).ti,ab,kf. or (("data extraction" or "data source*") and "study selection").ti,ab,kf. or ("search strategy" and "selection criteria").ti,ab,kf. or ("data source*" and "data synthesis").ti,ab,kf. or (medline or pubmed or embase or cochrane).ab. or ((critical or rapid) adj2 (review* or overview* or synthes*)).ti. or (((critical* or rapid*) adj3 (review* or overview* or synthes*)) and (search* or database* or data-base*)).ab. or (metasynthes* or meta-synthes*).ti,ab,kf. |
612522 |
|
6 |
limit 5 to ((english language or dutch) and yr="2000 -Current") |
2074 |
|
5 |
4 not (comment/ or editorial/ or letter/ or ((exp animals/ or exp models, animal/) not humans/)) |
3275 |
|
4 |
1 and 2 and 3 |
3481 |
|
3 |
exp appendectomy/ or exp Laparoscopy/ or appendectom*.ti,ab,kf. or exp Surgical Procedures, Operative/ or exp Specialties, Surgical/ or su.fs. or (surgical or surger* or operation* or operative).ti,ab,kf. |
5237182 |
|
2 |
exp Conservative Treatment/ or conservative.ti,ab,kf. or noninvasive.ti,ab,kf. or 'non invasive'.ti,ab,kf. or nonsurg*.ti,ab,kf. or 'non surg*'.ti,ab,kf. or nonoperati*.ti,ab,kf. or 'non operati*'.ti,ab,kf. or exp Drug Therapy/ or exp Infusions, Intravenous/ or intravenous.ti,ab,kf. or (drug adj2 (treat* or therap*)).ti,ab,kf. or exp Administration, Intravenous/ or exp Anti-Infective Agents/ or antibacterial*.ti,ab,kf. or (anti adj1 bacterial*).ti,ab,kf. or antibiotic*.ti,ab,kf. |
3783876 |
|
1 |
exp Appendicitis/ or appendicit*.ti,ab,kf. |
27045 |
Table of excluded studies
|
Reference |
Reason for exclusion |
|
Ehlers (2016) |
De Almeide Leite is a more recent published SR and includes the same studies. |
|
Emile (2022) |
De Almeide Leite is a more recent published SR and includes the same studies. |
|
Di Saverio (2014) |
De Almeide Leite is a more recent published SR and includes the same studies. |
|
Findlay (2016) |
De Almeide Leite is a more recent published SR and includes the same studies. |
|
Fitzmaurice (2012) |
Non-randomized study. |
|
Fitzmaurice (2011) |
Narrative review. |
|
Harnoss (2017) |
De Almeide Leite is a more recent published SR and includes the same studies. |
|
Herrod (2022) |
De Almeide Leite is a more recent published SR and includes the same studies. |
|
Köhler (2021) |
Narrative review. |
|
Flum (2020) |
Already included in SR of De Almeide Leite (2022). |
|
Hansson (2009) |
Non-randomized study. |
|
Liu (2011) |
De Almeide Leite is a more recent published SR and includes the same studies. |
|
Mason (2012) |
De Almeide Leite is a more recent published SR and includes the same studies. |
|
Poprom (2019) |
De Almeide Leite is a more recent published SR and includes the same studies. |
|
Rollins (2016) |
De Almeide Leite is a more recent published SR and includes the same studies. |
|
Monsell (2022) |
Non-randomized study. |
|
O’Leary (2021) |
Already included in SR of De Almeide Leite (2022). |
|
Park (2017) |
Wrong comparison. |
|
Sakran (2017) |
De Almeide Leite is a more recent published SR and includes the same studies. |
|
Sallinen (2016) |
De Almeide Leite is a more recent published SR and includes the same studies. |
|
Schumm (2020) |
Wrong comparison. |
|
Sugiura (2020) |
Wrong comparison. |
|
Varadhan (2009) |
De Almeide Leite is a more recent published SR and includes the same studies. |
|
Varadhan (2012) |
De Almeide Leite is a more recent published SR and includes the same studies. |
|
Yang (2019) |
De Almeide Leite is a more recent published SR and includes the same studies. |
|
Zagales (2022) |
De Almeide Leite is a more recent published SR and includes the same studies. |
|
Salminen (2015) |
Already included in SR of De Almeide Leite (2022) |
|
Salminen (2022) |
Already included in SR of De Almeide Leite (2022) |
|
Styrud (2006) |
Already included in SR of De Almeide Leite (2022) |
|
Talan (2017) |
Already included in SR of De Almeide Leite (2022) |
|
Talan (2022) |
Wrong comparison. |
|
Thompson (2022) |
Wrong comparison. |
|
Vons (2011) |
Already included in SR of De Almeide Leite (2022) |
Beoordelingsdatum en geldigheid
Publicatiedatum : 06-06-2024
Beoordeeld op geldigheid : 25-05-2024
Algemene gegevens
De ontwikkeling van deze richtlijnmodule werd ondersteund door het Kennisinstituut van de Federatie Medisch Specialisten (www.demedischspecialist.nl/kennisinstituut) en werd gefinancierd uit de Kwaliteitsgelden Medisch Specialisten (SKMS). De financier heeft geen enkele invloed gehad op de inhoud van de richtlijnmodule.
Samenstelling werkgroep
Voor het ontwikkelen van de richtlijnmodule is in 2021 een multidisciplinaire cluster ingesteld, bestaande uit vertegenwoordigers van alle relevante specialismen (zie hiervoor de Samenstelling van het cluster) die betrokken zijn bij gastro-enterologische chirurgie.
Belangenverklaringen
De Code ter voorkoming van oneigenlijke beïnvloeding door belangenverstrengeling is gevolgd. Alle clusterleden hebben schriftelijk verklaard of zij in de laatste drie jaar directe financiële belangen (betrekking bij een commercieel bedrijf, persoonlijke financiële belangen, onderzoeksfinanciering) of indirecte belangen (persoonlijke relaties, reputatiemanagement) hebben gehad. Gedurende de ontwikkeling of herziening van een module worden wijzigingen in belangen aan de voorzitter doorgegeven. De belangenverklaring wordt opnieuw bevestigd tijdens de commentaarfase.
Een overzicht van de belangen van de clusterleden en het oordeel over het omgaan met eventuele belangen vindt u in onderstaande tabel. De ondertekende belangenverklaringen zijn op te vragen bij het secretariaat van het Kennisinstituut van de Federatie Medisch Specialisten.
Clusterstuurgroep
Tabel 1. Gemelde (neven)functies en belangen stuurgroep
|
Clusterlid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Boermeester |
Chirurg |
|
Persoonlijke financiële belangen: Hieronder staan de beroepsmatige relaties met bedrijfsleven vermeld waarbij eventuele financiële belangen via de AMC Research B.V. lopen, dus institutionele en geen persoonlijke gelden zijn: Skillslab instructeur en/of spreker (consultant) voor KCI/3M, Smith&Nephew, Johnson&Johnson, Gore, BD/Bard, TELABio, GDM.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: Institutionele grants van KCI/3M, Johnson&Johnson, en New Compliance.
Intellectuele belangen en reputatie: Ik maak me sterk voor een 100% evidence-based benadering van maken van aanbevelingen, volledig transparant en reproduceerbaar. Dat is mijn enige belang in deze; geen persoonlijk gewin.
Overige belangen: Geen.
|
Geen restricties. |
|
Toorenvliet
|
Chirurg |
|
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: Geen.
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen. |
Geen restricties. |
|
van Rossem
|
Chirurg |
Geen. |
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: Geen.
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen.
|
Geen restricties. |
|
Faneyte
|
Chirurg |
Geen. |
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: Geen.
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen.
|
Geen restricties. |
|
Hollmann
|
Anesthesioloog |
|
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: ZonMw Doelmatigheid.
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen.
|
Geen restricties. |
|
Siersema
|
Maag-darm-leverarts |
Geen.
|
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: Geen.
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen.
|
Geen restricties. |
|
Beets-Tan
|
Radioloog |
Geen.
|
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: Geen.
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen.
|
Geen restricties. |
|
Doganer
|
Beleidsmedewerker Stichting Kind & Ziekenhuis |
Geen.
|
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: Geen.
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen.
|
Geen restricties. |
Clusterexpertisegroep
Tabel 2. Gemelde (neven)functies en belangen expertisegroep
|
Clusterlid |
Functie |
Nevenfuncties |
Gemelde belangen |
Ondernomen actie |
|
Hermanides
|
Internist |
|
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: Geen.
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen.
|
Geen restricties. |
|
Oosterhuis
|
Arts klinische chemie |
|
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: Financiering van twee lopende projecten alleen door de SKMS. Er zijn geen belangen bij de uitkomst van de projecten.
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen.
|
Geen restricties. |
|
Bruil
|
Maag-darm-leverarts
|
Geen.
|
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: Geen.
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen.
|
Geen restricties. |
|
Voermans
|
Maag-darm-leverarts
|
Geen.
|
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: Onderzoeks financiering/ ondersteuning door: - ZonMw - Boston Scientific - Zambon Nederland
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen.
|
Geen restricties. |
|
Verdonk
|
Maag-darm-leverarts
|
Geen.
|
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: COMBO studie.
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen.
|
Geen restricties. |
|
Andriesse
|
Arts-microbioloog
|
|
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: Geen.
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen.
|
Geen restricties. |
|
van Mens
|
Medisch microbioloog
|
|
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: Geen.
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen.
|
Geen restricties. |
|
de Reuver
|
Chirurg
|
Geen.
|
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: ZonMw.
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen.
|
Geen restricties. |
|
van de Laar
|
Chirurg
|
Geen.
|
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: Geen.
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen.
|
Geen restricties. |
|
van den Boom
|
Chirurg
|
Geen.
|
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: Geen.
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen.
|
Geen restricties. |
|
Sloots
|
Kinderchirurg
|
Geen.
|
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: Geen.
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen.
|
Geen restricties. |
|
Knijn
|
Patholoog
|
Geen.
|
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: Geen.
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen.
|
Geen restricties. |
|
Cobben
|
Radioloog
|
Allen betaald:
|
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: Geen.
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen.
|
Geen restricties. |
|
Maas
|
Radioloog
|
|
Persoonlijke financiële belangen: Geen.
Persoonlijke relaties: Geen.
Extern gefinancierd onderzoek: Geen.
Intellectuele belangen en reputatie: Geen.
Overige belangen: Geen.
|
Geen restricties. |
Inbreng patiëntenperspectief
Er werd aandacht besteed aan het patiëntenperspectief door de participatie van Stichting Kind & Ziekenhuis in de stuurgroep. De verkregen input is meegenomen bij het opstellen van de uitgangsvragen, de keuze voor de uitkomstmaten en bij het opstellen van de overwegingen. De conceptmodule is tevens te commentaar voorgelegd aan alle patiëntenorganisaties in de stuur- en expertisegroep. De eventueel aangeleverde commentaren zijn bekeken en verwerkt.
Methode ontwikkeling
Evidence based
Implementatie
Wkkgz & Kwalitatieve raming van mogelijke substantiële financiële gevolgen
Kwalitatieve raming van mogelijke financiële gevolgen in het kader van de Wkkgz
Bij de richtlijnmodule is conform de Wet kwaliteit, klachten en geschillen zorg (Wkkgz) een kwalitatieve raming uitgevoerd of de aanbevelingen mogelijk leiden tot substantiële financiële gevolgen. Bij het uitvoeren van deze beoordeling is de richtlijnmodule op verschillende domeinen getoetst (zie het stroomschema).
Uit de kwalitatieve raming blijkt dat er waarschijnlijk geen substantiële financiële gevolgen zijn, zie onderstaande tabel.
Tabel 3. Uitkomsten kwalitatieve raming
|
Module |
Uitkomst raming |
Toelichting |
|
Module 3.2 ‘Behandeling van simpele appendicitis bij volwassenen’
|
Geen financiële gevolgen |
Uit de toetsing volgt dat de aanbeveling(en) niet breed toepasbaar zijn (<5.000 patiënten) en zal daarom naar verwachting geen substantiële financiële gevolgen hebben voor de collectieve uitgaven.
|
Werkwijze
AGREE
Deze richtlijnmodule is opgesteld conform de eisen vermeld in het rapport Medisch Specialistische Richtlijnen 2.0 van de adviescommissie Richtlijnen van de Raad Kwaliteit. Dit rapport is gebaseerd op het AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II; Brouwers, 2010).
Need-for-update, prioritering en uitgangsvragen
Tijdens de need-for-update fase (September, 2021) inventariseerde het cluster de geldigheid van de modules binnen het cluster. Naast de partijen die deelnemen aan de stuur- en expertisegroep zijn hier ook andere stakeholders voor benaderd, zie onderstaande tabel.
Tabel 4. Partijen need-for-update
|
Partijen need-for-update |
||
|
Nederlands Huisartsen Genootschap |
Inspectie Gezondheidszorg en Jeugd |
Nederlandse Federatie van Universitair Medische Centra |
|
Nederlandse Vereniging van Ziekenhuizen |
Patiëntenfederatie Nederland |
Samenwerkende Topklinische opleidingsZiekenhuizen |
|
Verpleegkundigen & Verzorgenden Nederland |
Nederlandse Associatie Physician Assistants |
Zorginstituut Nederland |
|
Zelfstandige Klinieken Nederland |
Zorgverzekeraars Nederland |
|
Per module is aangegeven of deze geldig is, kan worden samengevoegd met een andere module, obsoleet is en kan vervallen of niet meer geldig is en moet worden herzien. Ook was er de mogelijkheid om nieuwe onderwerpen voor modules aan te dragen die aansluiten bij één (of meerdere) richtlijn(en) behorend tot het cluster. De modules die uit de need-for-update naar voren kwamen zijn besproken en geprioriteerd door leden van de stuur- en expertisegroep.
Voor de geprioriteerde modules zijn door de het cluster concept-uitgangsvragen herzien of opgesteld en definitief vastgesteld.
Uitkomstmaten
Na het opstellen van de zoekvraag behorende bij de uitgangsvraag inventariseerde het cluster welke uitkomstmaten voor de patiënt relevant zijn, waarbij zowel naar gewenste als ongewenste effecten werd gekeken. Hierbij werd een maximum van acht uitkomstmaten gehanteerd. Het cluster waardeerde deze uitkomstmaten volgens hun relatieve belang bij de besluitvorming rondom aanbevelingen, als cruciaal (kritiek voor de besluitvorming), belangrijk (maar niet cruciaal) en onbelangrijk. Tevens definieerde het cluster tenminste voor de cruciale uitkomstmaten welke verschillen zij klinisch (patiënt) relevant vonden.
Methode literatuursamenvatting
Een uitgebreide beschrijving van de strategie voor zoeken en selecteren van literatuur is te vinden onder ‘Zoeken en selecteren’ onder Onderbouwing. Indien mogelijk werd de data uit verschillende studies gepoold in een random-effects model. Review Manager 5.4 werd zo nodig gebruikt voor de statistische analyses. De beoordeling van de kracht van het wetenschappelijke bewijs wordt hieronder toegelicht.
Beoordelen van de kracht van het wetenschappelijke bewijs
De kracht van het wetenschappelijke bewijs werd bepaald volgens de GRADE-methode. GRADE staat voor ‘Grading Recommendations Assessment, Development and Evaluation’ (zie http://www.gradeworkinggroup.org/). De basisprincipes van de GRADE-methodiek zijn: het benoemen en prioriteren van de klinisch (patiënt) relevante uitkomstmaten, een systematische review per uitkomstmaat, en een beoordeling van de bewijskracht per uitkomstmaat op basis van de acht GRADE-domeinen (domeinen voor downgraden: risk of bias, inconsistentie, indirectheid, imprecisie, en publicatiebias; domeinen voor upgraden: dosis-effect relatie, groot effect, en residuele plausibele confounding).
GRADE onderscheidt vier gradaties voor de kwaliteit van het wetenschappelijk bewijs: hoog, redelijk, laag en zeer laag. Deze gradaties verwijzen naar de mate van zekerheid die er bestaat over de literatuurconclusie, in het bijzonder de mate van zekerheid dat de literatuurconclusie de aanbeveling adequaat ondersteunt (Schünemann, 2013; Hultcrantz, 2017).
Tabel 5. Gradaties voor de kwaliteit van wetenschappelijk bewijs
|
Definitie |
|
|
Hoog |
|
|
Redelijk |
|
|
Laag |
|
|
Zeer laag |
|
Bij het beoordelen (graderen) van de kracht van het wetenschappelijk bewijs in richtlijnen volgens de GRADE-methodiek spelen grenzen voor klinische besluitvorming een belangrijke rol (Hultcrantz, 2017). Dit zijn de grenzen die bij overschrijding aanleiding zouden geven tot een aanpassing van de aanbeveling. Om de grenzen voor klinische besluitvorming te bepalen moeten alle relevante uitkomstmaten en overwegingen worden meegewogen. De grenzen voor klinische besluitvorming zijn daarmee niet één op één vergelijkbaar met het minimaal klinisch relevant verschil (Minimal Clinically Important Difference, MCID). Met name in situaties waarin een interventie geen belangrijke nadelen heeft en de kosten relatief laag zijn, kan de grens voor klinische besluitvorming met betrekking tot de effectiviteit van de interventie bij een lagere waarde (dichter bij het nuleffect) liggen dan de MCID (Hultcrantz, 2017).
Overwegingen (van bewijs naar aanbeveling)
Om te komen tot een aanbeveling zijn naast (de kwaliteit van) het wetenschappelijke bewijs ook andere aspecten belangrijk en worden meegewogen, zoals aanvullende argumenten uit bijvoorbeeld de biomechanica of fysiologie, waarden en voorkeuren van patiënten, kosten (middelenbeslag), aanvaardbaarheid, haalbaarheid en implementatie. Deze aspecten zijn systematisch vermeld en beoordeeld (gewogen) onder het kopje ‘Overwegingen’ en kunnen (mede) gebaseerd zijn op expert opinion. Hierbij is gebruik gemaakt van een gestructureerd format gebaseerd op het evidence-to-decision framework van de internationale GRADE Working Group (Alonso-Coello, 2016a; Alonso-Coello 2016b). Dit evidence-to-decision framework is een integraal onderdeel van de GRADE methodiek.
De aanbevelingen geven antwoord op de uitgangsvraag en zijn gebaseerd op het beschikbare wetenschappelijke bewijs en de belangrijkste overwegingen, en een weging van de gunstige en ongunstige effecten van de relevante interventies. De kracht van het wetenschappelijk bewijs en het gewicht dat door het cluster wordt toegekend aan de overwegingen, bepalen samen de sterkte van de aanbeveling. Conform de GRADE-methodiek sluit een lage bewijskracht van conclusies in de systematische literatuuranalyse een sterke aanbeveling niet a priori uit, en zijn bij een hoge bewijskracht ook zwakke aanbevelingen mogelijk (Agoritsas, 2017; Neumann, 2016). De sterkte van de aanbeveling wordt altijd bepaald door weging van alle relevante argumenten tezamen. Het cluster heeft bij elke aanbeveling opgenomen hoe zij tot de richting en sterkte van de aanbeveling zijn gekomen.
In de GRADE-methodiek wordt onderscheid gemaakt tussen sterke en zwakke (of conditionele) aanbevelingen. De sterkte van een aanbeveling verwijst naar de mate van zekerheid dat de voordelen van de interventie opwegen tegen de nadelen (of vice versa), gezien over het hele spectrum van patiënten waarvoor de aanbeveling is bedoeld. De sterkte van een aanbeveling heeft duidelijke implicaties voor patiënten, behandelaars en beleidsmakers (zie onderstaande tabel). Een aanbeveling is geen dictaat, zelfs een sterke aanbeveling gebaseerd op bewijs van hoge kwaliteit (GRADE gradering HOOG) zal niet altijd van toepassing zijn, onder alle mogelijke omstandigheden en voor elke individuele patiënt.
Tabel 6. Sterkte van de aanbevelingen
|
Implicaties van sterke en zwakke aanbevelingen voor verschillende richtlijngebruikers |
||
|
|
Sterke aanbeveling |
Zwakke (conditionele) aanbeveling |
|
Voor patiënten |
De meeste patiënten zouden de aanbevolen interventie of aanpak kiezen en slechts een klein aantal niet. |
Een aanzienlijk deel van de patiënten zouden de aanbevolen interventie of aanpak kiezen, maar veel patiënten ook niet. |
|
Voor behandelaars |
De meeste patiënten zouden de aanbevolen interventie of aanpak moeten ontvangen. |
Er zijn meerdere geschikte interventies of aanpakken. De patiënt moet worden ondersteund bij de keuze voor de interventie of aanpak die het beste aansluit bij zijn of haar waarden en voorkeuren. |
|
Voor beleidsmakers |
De aanbevolen interventie of aanpak kan worden gezien als standaardbeleid. |
Beleidsbepaling vereist uitvoerige discussie met betrokkenheid van veel stakeholders. Er is een grotere kans op lokale beleidsverschillen. |
Organisatie van zorg
Bij de ontwikkeling van de richtlijnmodule is expliciet aandacht geweest voor de organisatie van zorg: alle aspecten die randvoorwaardelijk zijn voor het verlenen van zorg (zoals coördinatie, communicatie, (financiële) middelen, mankracht en infrastructuur). Randvoorwaarden die relevant zijn voor het beantwoorden van deze specifieke uitgangsvraag zijn genoemd bij de overwegingen. Meer algemene, overkoepelende, of bijkomende aspecten van de organisatie van zorg worden behandeld in de module Organisatie van zorg.
Commentaar- en autorisatiefase
De conceptrichtlijnmodule werd ter commentaar voorgelegd aan alle partijen die benaderd zijn voor de need-for-update fase. De commentaren werden verzameld en besproken met het cluster. Naar aanleiding van de commentaren werd de conceptrichtlijnmodule aangepast en definitief vastgesteld door het cluster. De definitieve richtlijnmodule werd voorgelegd ter autorisatie aan de partijen die beschreven staan onder het kopje geldigheid en onderhoud (zie verantwoording).