Hydratie en complicaties
Uitgangsvraag
Welke hydratiestrategie dient te worden toegepast bij patiënten die intravasculair jodiumhoudend contrastmiddel (CM)-toediening ondergaan en een hoog PC-AKI risico hebben?
Subvragen
- Is er een significant verschil in de incidentie van PC-AKI bij hydratie versus geen hydratie?
- Is er een significant verschil in de incidentie van PC-AKI bij orale versus intraveneuze pre- en posthydratie?
- Is er een significant verschil in de incidentie van PC-AKI bij intraveneuze NaCl versus NaHCO3?
- Is er een significant verschil in de incidentie van PC-AKI bij intraveneuze prehydratie (alleen) versus pre- en posthydratie (gecombineerd)?
- Is er een significant verschil in de incidentie van PC-AKI bij patiënten die gecontroleerde diurese ondergaan versus standaard hydratieschema’s?
Aanbeveling
Voor patiënten met eGFR <30 ml/min/1,73m2 die intravasculair jodiumhoudend CM-toediening ondergaan kan één van de volgende opties worden toegepast:
- Pas prehydratie toe met NaHCO3 1,4%, 3ml/kg/uur gedurende 1 uur vooraf aan CM-toediening.
- Pas pre- en posthydratie toe met NaHCO3 1,4%, 3ml/kg/uur (of 250 mL in totaal) gedurende 1 uur vooraf aan CM-toediening en 1ml/kg/h (of 500mL in totaal) gedurende 6 uur na CM-toediening.
Pas geen hydratie met gecontroleerde diurese toe ter preventie van PC-AKI bij patiënten die (cardiale) angiografie met of zonder interventie ondergaan, tenzij in studieverband.
Pas geen orale hydratie toe als enige preventie van PC-AKI.
Overwegingen
All studies
The number of patients with eGFR <30 ml/min/1.73m2 is absent or very low in all described studies. No RCT has been publshed focusing on patients with eGFR <30 ml/min/1.73m2 only, and subanalyses for this group within other RCTs were not performed. Furthermore, independent of eGFR, all patients receiving CM should have a normal hydration status. Dehydration should be corrected at all times before administering CM.
Hydration versus no hydration
The most valuable new information comes from the study from Nijssen, 2017. This prospective randomised RCT in 603 patients with eGFR 30-59 ml/min/1.73m2, shows that the incidence of PC-AKI is het same in the group receiving pre- and post-hydration with NaCl 0.9% compared to the group withholding hydration, 2.7% versus 2.6% respectively (one-sided 95% CI -2.25 to 2.06). Further analyses showed no significant differences in the incidence of PC-AKI between patients receiving iv NaCl 0.9% and those not receiving prophylaxis in the subgroups with or without diabetes; eGFR 30-44 ml/min/1.73m2 or eGFR 45-59 ml/min/1.73m2; intra-arterial contrast administration or intra-venous contrast administration; and undergoing an interventional or diagnostic procedure. As this study has been conducted in the Netherlands, these results are highly applicable to this guideline.
Oral versus intravenous hydration
The quality of evidence for the effectivity of oral hydration for the prevention of PC-AKI is low. Furthermore, the oral intake of patients could not be quantified and could therefore lead to PC-AKI due to lack of adherence to oral hydration instructions. Therefore, it is the recommendation of the working group that oral hydration should not be used in the prevention of PC-AKI. However, the encouragment of patients using oral fluids unrestrictedly on the day of CM exposure, besides other preventive measures, is advisable.
Saline versus bicarbonate
Intravenous administration of NaCl 0.9% before, during and after CM administration will produce an infusion rate-dependent increase in tubular fluid volume, reduction in CM intratubular concentration, and slight increases in tubular pH. The lower tubular concentrations of CM lead to reduced formation of reactive oxygen species (ROS) and therefore to reduced toxicity to tubular cells.
Infusion of NaHCO3 1.4% has the same effects as NaCl 0.9% infusion with the additional benefit of a substantial increase in the bicarbonate anion buffer throughout the renal tubule. Higher pH is known to decrease cellular apoptosis in the setting of ROS formation. Prehydration with NaHCO3 will raise the proximal tubular bicarbonate anion and pH levels close to those found in blood. Maintainance of NaHCO3 infusion will keep the bicarbonate anion levels raised while the CM is excreted. (Burgess, 2014)
For descriptive purposes, three hydration schedules have been described in the literature:
- long schedule: 1ml/kg/h for 12h pre and for 12h post CM administration;
- short schedule: 3ml/kg/h for 1h pre and 1ml/kg/h 6h post CM administration;
- ultra-short schedule: 3ml/kg/h NaHCO3 1.4% for 1h pre-CM administration (Kooiman, 2014).
The landmark paper giving the first evidence on the effectiveness of NaHCO3 pre- and post hydration was published in 2004 (Merten, 2004). This group describes an RCT consisting of 119 patients with a sCr ≥ 97,2 µmol/l undergoing either cardiac catheterizations (n=97) or CT (n=9) or other procedures involving intravascular contrast administration (n=13). Patients were randomly assigned to receive either 154mEq/l NaHCO3 or 154mEq/l NaCl, both in dextrose 5% in water. Both groups received the fluid mixture at a rate of 3ml/kg/h for 1 hour pre CM injection and at a rate of 1ml/kg/h for 6 hours after CM injection. PC-AKI was defined as a rise of sCr ≥25% within 2 days after CM administration. The incidence of PC-AKI in the NaHCO3 group was 1.7% (1 of 60) and 13.6% (8 of 59) in the NaCl group.
The positive results of this relatively short NaHCO3 hydration schedule triggered a boom in RCTs comparing NaHCO3 vs. NaCl. The mixture used in the landmark paper is not commercially available. The most resembling commercially available concentrations are NaHCO3 1.4% (i.e. 166 mEq/L NaHCO3) and NaCl 0,9%. Some RCTs used the commercially available solutions, others used the mixture described by Merten (2004).
Many studies are now available comparing the effect of bicarbonate hydration to saline hydration on the risk of PC-AKI. However, these studies are very heterogenous in the hydration solutions, volumes and schedules. Also, sample size is often small and confidence intervals are wide, also due to the low incidence of PC-AKI. Therefore, the conclusions on the comparison of bicarbonate and saline in terms of prevention of CI-AKI are not certain, but overall, no difference in PC-AKI risk is found. Also, when considering the literature results, no preference can be given for a certain hydration schedule.
Since bicarbonate can be given just 1 hour prior to CM administration and thus considered more patient-friendly and less burdensome on the healthcare system, the Working Group expresses a preference for this type of bicarbonate hydration.
The literature on effectiveness of hydration schedules for prevention of PC-AKI would greatly benefit from optimized study designs with properly defined control populations (e.g. supported by propensity score matching) as has been done for PC-AKI risk stratification studies when CM is injected intravenously or for hydration in CT pulmonary angiography.
Although the bicarbonate prehydration volume is relatively low, the risk of pulmonary fluid overload or congestive heart failure should be considered and weighed against its potential benefit, especially in patients on chronic dialysis and with poor cardiac function and critical illness related fluid overload.
Note: In critically ill patients lactated Ringer’s, a balanced crystalloid, may be preferable to saline hydration because of it somewhat lower osmolality and the reduced chance of hyperchloremic acidosis, which may contribute to the preservation of renal function.
Hydration with controlled diuresis
The ratio behind this technique is to increase renal blood flow and urinary output in a controlled environment, based on patient’s parameters, such as central venous pressure, left ventricular end diastolic pressure or urinary output. The amount of additional intravenous fluids and, if necessary a low dose diuretic, is individualized by the abovementioned parameters. These techniques can only be applied in an in-patient setting as intravenous or intra-arterial catheters are necessary, combined with a urinary catheter for monitoring urinary production. This makes these techniques applicable for a subgroup of patients. The Working Group thinks that controlled diuresis is a promising new invasive strategy to prevent PC-AKI in hospitalized patients undergoing (cardiac) angiography with or without intervention. Which technique is optimal is unknown. More information and research is needed before reliable conclusions can be drawn regarding the effectiveness and preferred type of controlled diuresis, or its application in an outpatient setting. Therefore, the Working Group recommends that, for now, this technique should be reserved for a research setting only.
Onderbouwing
Achtergrond
When it comes to prevention of PC-AKI, the cornerstone is hydration (volume expansion). In the literature, many hydration schedules, hydration fluids and routes of administration have been described. These schedules have been rubricated into the 5 above mentioned categories.
Conclusies
|
Low GRADE |
There is a low level of evidence that withholding hydration is as effective as single bolus hydration of 250ml NaHCO3 in the prevention of PC-AKI prior to computed tomography pulmonary angiography with intravenous iodine-containing CM administration for suspected pulmonary embolism.
(Kooiman, 2014) |
|
Moderate GRADE |
There is a moderate level of evidence that no hydration is non-inferior in preventing PC-AKI compared with intravenous pre- and post- hydration in patients with an eGFR between 30-59 ml/min/1.73m2.
(Nijssen, 2017) |
|
Low GRADE |
There is a low level of evidence that oral hydration is as effective as intravenous hydration in the prevention of PC-AKI in patients receiving intra-arterial iodine-containing contrast medium administration.
(Cho, 2010) |
|
|
No evidence was found regarding the effectiveness of oral hydration versus intravenous hydration in the prevention of PC-AKI in patients receiving intravenous iodine-containing contrast medium. |
|
Low GRADE |
Bicarbonate and saline pre- and post-hydration are similar in the prevention of PC-AKI independent on the administered schedules.
(Adolph, 2008; Boucek, 2013; Brar, 2008; Briguori, 2007; Castini, 2010; Chong, 2014; Gomes, 2012; Hafiz, 2012; Klima, 2011; Koc, 2013; Lee, 2011; Maioli, 2008; Masuda, 2007; Merten, 2004; Nieto Rios, 2014; Ozcan, 2007; Ratcliffe, 2009; Recio-Mayoral, 2007; Shavit, 2009; Solomon, 2015) |
|
Moderate GRADE |
There is a moderate level of evidence that administration of 250ml NaHCO3 1.4% prehydration is as effective as 1000ml NaCl 0.9% prehydration and 1000ml NaCl 0.9% posthydration in the prevention of PC-AKI in CT.
(Kooiman, 2014) |
|
Low GRADE |
There is a low level of evidence that hydration with controlled diuresis is more effective than intravenous hydration alone in the prevention of PC-AKI in patients who underwent cardioangiography procedures with intra-arterial iodine-containing contrast medium administration.
(Barbanti, 2015; Brar, 2014; Briguori, 2011; Marenzi, 2012; Qian, 2016; Usmiani, 2016; Visconti 2016) |
|
|
No evidence was found regarding the effectiveness of hydration with controlled diuresis versus intravenous hydration in the prevention of PC-AKI in patients who underwent CT with intravenous iodine-containing contrast medium administration. |
Samenvatting literatuur
1. Hydration versus no hydration:
Description of studies
Six RCTs were found for this comparison (Chen, 2008; Jurado-Roman, 2015; Kooiman 2014; Luo, 2014; Maioli, 2011; Nijssen, 2017).
Three of these involved comparisons for patients undergoing primary percutaneous intervention (PCI). Both Jurado-Roman, 2015, Luo, 2014 and Maioli, 2011 included myocardial infarction patients needing immediate PCI. In all 3 studies, the majority of patients had eGFR >60 ml/min/1.73m2, therefore these studies were excluded in the analysis.
Chen, 2008 used half saline (NaCl 0.45%) as hydration fluid and only the patients with impaired kidney function received NAC orally. For these two reasons, this study was excluded form the analysis. Thus only two studies were included in the literature analysis.
Kooiman, 2014 described 138 patients with eGFR <60 ml/min/1.73m2 undergoing chest CT for suspected pulmonary embolism. Sixty-seven patients received no hydration and the remaining 71 patients received 250ml NaHCO3 1.4% within one hour prior to CT.
Nijssen, 2017 included 660 high risk patients (≥18y), as indicated by the local (Dutch) and European guidelines, with an eGFR of 30-59 mL per min/1.73m2 undergoing an elective procedure requiring ionidated contrast material which were randomly assigned to: (1) intravenous NaCl (0.9% NaCl 3-4 ml/kg/h during 4 hrs pre- and post-contrast) (n=332) or (2) no prophylaxis (n=328). Of Note: 48% of patients received the long hydration protocol, 12 hours pre- and 12 hours post-contrast.
Results
Kooiman, 2014 reported a PC-AKI incidence of 8.1% in the group withholding hydration versus 7.1% in the group with 1-hour pre-hydration with 250ml NaHCO3, RR: 1.29 (95%CI: 0.41 to 4.03). None of the PC-AKI patients developed need for dialysis.
Nijssen, 2017 reported that PC-AKI occurred in eight (2.7%) of 296 intravenously hydrated patients and in eight (2.6%) of the no-prophylaxis patients, with a nonsignificant absolute difference in proportions of -0.1% (one-sided 95% CI: -2.25 – 2.06, one-tailed p=0.471).
Quality of evidence
The level of evidence was graded as low for Kooiman, 2014 due to imprecision and indirectness (only patients with suspicion of pulmonary embolism were included); thus the evidence was downgraded by 2 levels. The level of evidence was graded as moderate for Nijssen, 2017, downgraded 1 level, due to imprecision. Power analysis indicated that 1300 patients would give a reasonable (80%) chance of detecting a difference between groups (as estimated using the expected H+ group CIN incidence 2.4%, a non-inferiority margin 2.1%, and given a conventional level of alpha (0.05), only 660 patients were included. (Nijssen, 2017)
2. Oral versus intravenous hydration:
Description of studies
A total of nine RCTs on this subject have been published, but only two were considered suitable to be included in this literature summary. Four RCTs included patients with normal kidney function (Trivedi, 2003; Kong, 2012; Akyuz, 2014; Martin-Moreno, 2015). Two RCTs described a mixture of oral and intravenous hydration, compared to intravenous hydration alone (Taylor, 1998; Lawlor 2007). One RCT did not define PC-AKI (Wrobel, 2010), only describing serum creatinine changes. The last excluded RCT described 4 research arms, three with intravenous hydration and one with extra NaCl orally, but no extra fluid orally. Therefore, this RCT was excluded (Dussol, 2006). One RCT (Cho, 2010) was condidered suitable for inclusion in the literature summary.
Cho, 2010 the RCT using both pre- and post hydration consisted of 91 patients with sCr >97,2 µmol/l or eGFR <60 ml/min/1.73m2 undergoing elective CAG. They were randomly assigned into 4 groups: A, NaCl 154mEq (0.9%)/l 3ml/kg/h 1 hour pre and 1ml/kg/h 6 hours post CM. B. NaHCO3 154mEq/l, same schedule as NaCl. C. 500ml of water, 4-2 hours pre CM administration, followed by 600ml of water post contrast administration. D, C + 3.9g oral NaHCO3 pre CM and 1.95g oral NaHCO3 post CM.
Results
Cho, 2010 also found no significant difference in the incidence of PC-AKI in all 4 groups; A 22.2%, B 9.5%, C 4.5% and D 4.8% (p>0.05).
Quality of evidence
For the comparison oral versus intravenous hydration in all patients the level of evidence was graded as low due to imprecision and heterogeniety of included studies.
3. Saline (sodium chloride) versus sodium bicarbonate hydration:
Description of studies
Depending on the design, the RCTs comparing sodium to bicarbonate hydration were categorized into several groups:
- Short schedule NaHCO3 vs. short schedule NaCl in patients with impaired kidney function undergoing coronary angiography (CAG) and/or PCI. A total of 10 RCTs (Adolph, 2008; Boucek, 2013; Brar, 2008; Gomes, 2012; Manari, 2014; Masuda, 2007; Ozcan, 2007; Ratcliffe, 2009; Recio-Mayoral, 2007; Solomon 2015) with 2,408 patients were identified, that compared bicarbonate and saline hydration in a similar hydration scheme for coronary angiography. All the studies were performed in patients with impaired kidney function;
- Short schedule NaHCO3 vs. long schedule NaCl (1ml/kg/h for 12h pre- and 12h post-CM administration) in patients with impaired kidney function undergoing CAG and/or PCI. A total of 9 RCTs (Briguori, 2007; Castini, 2010; Hafiz, 2012; Klima, 2012; Koc 2013 Lee, 2011; Maioli, 2008; Nieto Rios, 2014; Shavit, 2009) with 3,026 patients were identified that compared bicarbonate hydration to saline pre- and posthydration (1ml/kg, 12hour pre- and post) for coronary angiography;
- All other hydration schedules comparing bicarbonate plus saline to saline or to bicarbonate only. Four RCTs (Chong, 2015; Motohiro, 2011; Tamuro, 2009; Ueda, 2011) with 358 patients compared bicarbonate to saline hydration with divergent hydration schemes for coronary angiography, like adding a bolus NaHCO3 to saline hydration or exchanging saline by NaHCO3 hydration for multiple hours;
- One RCT compared in a non-inferiority trial, a 1-hour schedule of 250ml NaHCO3 1.4% versus 1000 ml NaCl 0,9% in 4-12h pre- and 4-12h post-CM administration in 548 CT patients. (Kooiman, 2014).
Results
Depending on the design, the RCTs comparing sodium to bicarbonate hydration were categorized into several groups:
- Short schedule NaHCO3 (3ml/kg/h 1 hour pre and 1ml/kg/h 6 hours post CM administration) vs. short schedule NaCl in patients with impaired kidney function undergoing CAG and/or PCI. A total of 10 RCTs with 2,408 patients and 288 PC-AKI events were indentified (Adolph, 2008; Boucek, 2013; Brar, 2008; Gomes, 2012; Manari, 2014; Masuda, 2007; Ozcan, 2007; Ratcliffe, 2009; Recio-Mayoral, 2007; Solomon 2015). No significant difference was found between patients that underwent bicarbonate versus saline hydration: Risk Ratio (RR): 0.88 (95% CI: 0.51 – 1.50), p=0.63, I2=60%, as shown in Figure 1;
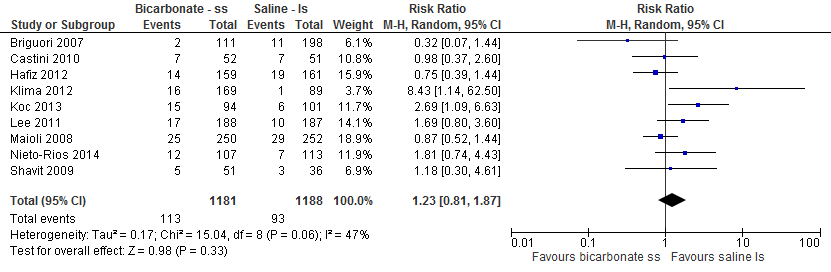
- Short schedule NaHCO3 (3ml/kg/h 1 hour pre and 1ml/kg/h 6 hours post CM administration) vs. long schedule NaCl (1ml/kg/h 12 hours before and after CM administration) in patients with impaired kidney function undergoing CAG and/or PCI. A total of 9 RCTs (Briguori, 2007; Castini, 2010; Hafiz, 2012; Klima, 2012; Koc 2013; Lee, 2011; Maioli, 2008; Nieto Rios, 2014; Shavit, 2009) with 2,994 patients and 272 PC-AKI events were identified that compared bicarbonate hydration to saline pre- and posthydration (1ml/kg, 12hour pre- and post) for coronary angiography. No significant difference was found between patients that underwent bicarbonate versus saline hydration: Risk Ratio (RR): 1.23 (95% CI: 0.81 – 1.87), p=0.33, I2=47% as shown in Figure 2;
- All other hydration schedules comparing bicarbonate plus saline to saline or to bicarbonate only. A total of 4 RCTs (Chong, 2015; Motohiro, 2011; Tamura, 2009; Ueda, 2011) with 668 patients and 58 PC-AKI cases, were considered suitable for this literature summary. The studies were considered too heterogenous in terms of hydration fluid content and hydration schemes in control group and treatment group to be considered for pooling. Chong, 2015 reported that PC-AKI incidences were 10/153 (6.5%) in the group receiving NaCl plus NAC, and 16/151 (10.6%) in the group bicarbonate plus NAC. The difference in PC-AKI incidence between groups was not significant. Motohiro, 2011 reported that 2/78 patients in the bicarbonate plus saline group versus 10/77 in the standard hydration group (RR: 0.20, 95% CI: 0.04 to 0.87) developed PC-AKI, thus the incidence of PC-AKI was lower in the combination group. Tamura, 2009 also reported lower rates of PC-AKI in the bolus group: 1/72 versus 9/72 (RR: 0,11; 95% CI: 0.01 to 0.85. The results of Ueda, 2011 were similar, although the difference in incidence of PC-AKI was not statistically significant: 2/30 versus 8/29 PC-AKI cases; RR: 0.24 (95% CI: 0.06 to 1.04);
- Kooiman, 2014 reported a PC-AKI incidence of 4.1% in CT patients receiving 250ml NaHCO3 (ultrashort schedule) precontrast versus 5.1% (p=0.23) receiving pre- and post-CM hydration with NaCl 0,9%. No patients developed a need for dialysis.
The risk of mortality, dialysis requirement and cardiovascular complications of hydration (such as pulmonary oedema) are shown in Table 1 for all the saline versus sodium bicarbonate hydration comparisons. The number of adverse events was often not reported, and when reported was low. In the Kooiman 2014 study, mentioned in the paragraph above, Acute heart failure due to volume expansion (based on the treating physician’s clinical judgement) occurred in none of the patients in the NaHCO3 group versus 6 of 281 patients in the saline group (p = 0.03). Consequently, NaCl 0,9% hydration was prematurely stopped in 1 of 281 patients. (Kooiman, 2014).
Quality of evidence
For the comparison bicarbonate versus saline, the level of evidence was graded as low (downgraded by 2 levels) due toe heterogeniety and imprecision. For the comparison bicarbonate bolus versus saline bolus hydration for emergency angiography, followed by bicarbonate hydration in both groups, the level of evidence was downgraded with one more level for imprecision (very low number of events).
4. Pre-hydration only versus pre- and posthydration:
Description of studies
One RCT compared in a non-inferiority trial, a 1-hour schedule of 250ml NaHCO3 1.4% versus 1000 ml NaCl 0,9% in 4-12h pre- and 4-12h post-CM administration in 548 CT-patients. (Kooiman, 2014).
Results
Kooiman, 2014 reported a PC-AKI incidence of 4.1% in CT patients receiving 250ml NaHCO3 (ultrashort schedule) pre-contrast versus 5.1% (p=0.23) receiving pre- and post-CM hydration with NaCl 0,9%. No patients developed a need for dialysis.
Quality of evidence
This non-inferiority study from the Netherlands has sufficient number of patients, therefore the evidence was graded as moderate.
5. Hydration with controlled diuresis:
Description of studies
Five Italian studies, all RCTs, describe the same technique, consisting of an extracorporeal circuit for continuous fluid infusion, combined with a Foley catheter for measuring urinary production (Barbanti, 2015; Briguori, 2011; Marenzi, 2012; Usmiani, 2016; Visconti, 2016) in respectively 112, 292, 170, 123, and 48 patients. This system is capable of delivering sterile replacement solution in an amount matched to the volume of urine produced, thereby avoiding hypovolemia and fluid overload. It displays urine and replacement volume and alerts to replace the fluid bag or drain the urine bag. After an initial bolus of 250ml NaCl 0.9% infused over 30 minutes, patients receive furosemide, 0.25mg/kg, to achieve a urinary flow of at least 300ml/h. Once this is achieved, the procedure is performed. The system keeps urinary flow >300ml/h for the next 4 hours, balancing between more NaCl and low dose furosemide.
Two of these three papers describe patients undergoing CAG and/or PCI (Marenzi, 2012; Usmiani, 2016), two papers describe patients undergoing Transcatheter Aortic Valve Implantation (TAVI) (Barbanti, 2015; Visconti, 2016) and one describes a mixed group of CAG and peripheral angiography (Briguori, 2011). All patients had eGFR <60 ml/min/1.73m2, in one paper <30 ml/min/1.73m2 (Briguori, 2011). The control group of each study had a different hydration schedule (saline versus bicarbonate versus a combination of both). Therefore, pooling of the studies was not possible due to heterogeneity.
Regarding the control group, Briguori, 2011 used 154 mEq/L of sodium bicarbonate in dextrose and water, mixed in the hospital pharmacy by adding 154mL of 1000 mEq/L sodium bicarbonate (i.e. sodium bicarbonate 8.4%) to 846 mL of 5% dextrose in water (D5W), slightly diluting the dextrose concentration to 4.23%. The initial intravenous bolus was 3 mL/kg per hour for at least 1 hour before contrast injection. Then, all patients received the same fluid at a rate of 1 mL/kg per hour during contrast exposure and for 6 hours after the procedure. All patients enrolled in this group received NAC orally at a dose of 1200 mg twice daily the day before and the day of administration of the contrast agent (for a total of 2 days). In this group, an additional NAC dose (1200 mg diluted in 100 mL normal saline) was administered intravenously during the procedure. The total NAC dose was 6g.
The control group of Marenzi, 2012 recieved a continuous intravenous infusion of isotonic saline at a rate of 1 ml/kg/h (0.5 ml/kg/h in case of left ventricular ejection fraction <40%) for at least 12 h before and 12 h after the procedure.The control group of Usmiani, 2016 recieved 1000 mL isotonic saline i.v. administration 12 h before procedure (rate-adjusted according to LVEF: 20– 40mL/h if LVEF<30%, 80–120 mL/h if LVEF 30–50%, 200 mL/h if LVEF >50%), plus 3 mL/kg/h sodium bicarbonate 1.4% solution by i.v. infusion for 1 h before procedure, plus 5000mg of Vitamin C and 1200mg NAC administered orally. After the procedure the patients received 1mL/kg/h sodium bicarbonate 1.4% solution IV for 6 hours, plus 5000mg of vitamin C and 1200mg NAC administered orally on the following day.
Barbanti, 2015 included 112 patients undergoing Transcatheter Aortic Valve Implantation (TAVI) who were randomly assigned to either the controlled diuresis group (n=56) or the control group (intravenous saline solution at a rate of 1 ml/kg/h 12 h before TAVI, during contrast exposure, and for 6 h after the procedure).
Viconti, 2016 describes also a group of patients undergoing TAVI (n=48) with either controlled diuresis or bicarbonate schedule (same schedule as Briguori, 2011). In total, 48 patients were assigned (non-randomly) to the RenalGuard therapy group (n=22) or the control group (n=26). Because the above-mentioned studies used different hydration schemes and methods, the studies could not be pooled.
Brar, 2014 described a slightly different approach: during CAG, a left ventricular catheter was placed in order to measure left ventricular end-diastolic pressure. This was done in 178 patients with eGFR <60 ml/min/1.73m2 and one or more additional risk factors, such as diabetes, congestive heart failure, hypertension and age >75 years. The control group consisted of 172 patients with the same characteristics, undergoing the same procedure. Both groups received a bolus infusion, NaCl 0.9%, 3ml/kg/h, 1 hour pre CAG. The control group received the same fluid at the same rate for 4 hours post CAG. The rate of post contrast fluid in the research group was dependent on the left ventricular end-diastolic pressure: <13mmHg 5ml/kg/h, 13 to 18mmHg 3ml/kg/h and >18mmHg 1.5ml/kg/h.
Another approach, described by Qian, 2016, is invasively measuring central venous pressure (CVP) and CVP-guided fluid administration in 264 patients. CVP <6mmHg 3ml/kg/h, CVP 6-12mmHg 1.5ml/kg/h, CVP>12mmHg 1ml/kg/h NaCl 0.9% 6 hours pre and 12 hours post CM administration. The control group received NaCl 1ml/kg/h 6 hours pre and 12 hours post CM administration. All patients were scheduled for CAG and/or PCI, had an eGFR 15-60 ml/min/1.73m2 and LVEF <50% (Qian, 2016).
Results
Briguori, 2011, Marenzi, 2012 and Usmiani, 2015 all reported a significantly lower incidence of PC-AKI in patients who received controlled diuresis. Briguori, 2011 found an incidence of PC-AKI of 11% in the forced diuresis group versus 20.5% in the control group (p=0.025) in patients with an eGFR <30mL/min/1.73m2. After 1 month, mortality was similar in the intervention (6/146) and control (6/146) group, p=0.99; need for dialysis arose in 7/146 patients in the control group versus 1/146 in the intervention group, p=0.03.
Marenzi, 2012 found an incidence of PC-AKI of 4,6% in the forced diuresis group versus 18% in the control group (p=0.005). In-hospital mortality was similar in the intervention (1/87) and control (2/82) group, p=0.53. Need for dialysis arose in 1/87 patients in the intervention group versus 3/83 in the control group, p=0.29.
Usmiani, 2016 found an incidence of PC-AKI of 7% in the forced diuresis group versus 25% in the control group (p=0.01). One-year mortality was not significantly different in the intervention (4/59) and control (8/65) group, p=0.46. Need for dialysis arose in 0/59 patients in the intervention group versus 2/65 in the control group, (p-value not reported).
Barbanti reported that the incidence of CI-AKI was lower in the controlled diuresis group compared to the control group (intravenous), controlled diuresis: 4/56 (5.4%) vs control: 13/56 (13.3%) (p=0.014).
Visconti, 2016 reported that PC-AKI occurred in 10/26 (38.5%) patients in the control group and in 1/22 (4.5%) patients in the RenalGuard group (p=0.005, odds ratio [OR] 0.076, 95% confidence interval [CI]: 0.009-0.66).
Brar, 2014 described that PC-AKI occured in 16.3% of the patients in the control group vs. 6.7% in the research group (p=0.005). After 6 months, mortality was lower in the intervention (1/196) compared to the control (8/200) group, p=0.037. Need for dialysis arose in 1/196 patients in the intervention group versus 4/200 in the control group, p=0.37.
Qian, 2016 reported that PC-AKI occured in 15.9% in the CVP group vs. 29.5% in the standard hydration group (p=0.006). Need for dialysis arose in 4/134 patients in the intervention group versus 13/135 in the control group, p=0.019. Acute pulmonary edema occurred in 5/134 patients in the intervention group versus 4/135 in the control group, p=0.50. Mortality rates were not reported.
Quality of evidence
For the comparison controlled diuresis versus IV hydration in all patients the level of evidence was graded as low due to imprecision and heterogeniety of included studies.
Figure 1 Pooled analysis of PC-AKI risk in patients receiving short schedules of hydration with either bicarbonate or saline for CAG/PCI
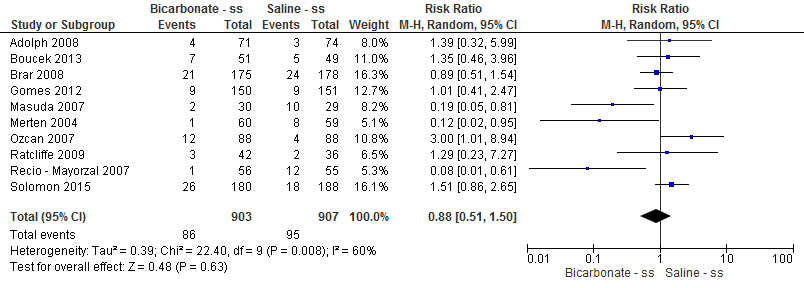
Figure 2 Pooled analysis of PC-AKI risk in patients receiving short schedules for bicarbonate versus long schedule for saline for CAG/PCI.
Zoeken en selecteren
To answer our clinical question a systematic literature analysis was performed for the following research question:
What type of hydration reduces the risk of contrast-associated acute kidney injury best in patients undergoing radiological examinations with intravascular contrast administration?
P (patient category) Patients undergoing radiological examinations with iodine-containing contrast media.
I (intervention) Hydration with NaCl i.v., hydration with bicarbonate, oral hydration, hydration, pre- and posthydration.
C (comparison) One of the forms of hydration described above or no hydration.
O (outcome) Post-contrast acute kideny injury (PC-AKI), start dialysis, decrease in residual kidney function, cost-effectivity.
Relevant outcome measures
The working group considered PC-AKI, mortality, start dialysis, decrease in residual kidney function, critical outcome measures for the decision making process and adverse effects of hydration and cost-effectivity important outcome measures for the decision-making process. The working group defined the outcome measure PC-AKI as described in the introduction of the Guideline.
A difference of at least 10% in relative risk was defined as a clinically relevant difference; by expert opinion of the working group (no literature was available to substantiate the decision). To illustrate, if PC-AKI occurs with an incidence of 10% in the patient population, a difference of 10% of relative risk would mean a difference of 1% in absolute risk. Thus, the number needed to treat would be 100, ergo: a doctor would need to treat 100 patients to prevent one case of PC-AKI. When the incidence of PC-AKI is 5%, a difference of 10% in relative risk would mean a difference of 0.5% in absolute risk, and a number needed to treat of 200.
Search and select (method)
The databases Medline (OVID), Embase and the Cochrane Library were searched from January 2000 to 17th of June 2015 using relevant search terms for systematic reviews (SRs), randomized controlled trials (RCTs) and observational studies (OBS). Search terms are shown in the Appendix. The literature search procured 858 hits: 183 SRs, 572 RCTs and 103 OBS. An update of the search on April 14th 2017 retrevied an additional 138 studies.
Studies were selected based on the following criteria:
- Adult patients who underwent radiological examination using contrast media (including radiological examination during percutaneous angiography)
- Patients with impaired kidney function, at least eGFR <60 ml/min/1.73m2
- Hydration types: hydration with NaCl i.v., hydration with bicarbonate, oral hydration, pre-hydration, pre- and posthydration
- At least one of the outcome measures was described: Post-contrast acute kidney injury (PC-AKI), Contrast-induced nephropathy (CIN)/contrast-induced acute kidney injury (CI-AKI), start dialysis, decrease in residual kidney function, adverse effects of hydration (overfilling, intensive care unit admittance, mortality), cost-effectivity
- Follow-up time after hydration was at least 48 hours
Based on title and abstract a total of 47 studies were initially selected, and a total of 17 studies based on the updated search (64 in total). After examination of full tekst a total of 19 + 10 (29 in total) studies were excluded and 28 + 7 studies definitely included in the literature summary.
Results
Thirty-five studies were included in the literature analysis, the most important study characteristics and results were included in the evidence tables. The evidence tables and assessment of individual study quality are included.
Referenties
- Adolph E, Holdt-Lehmann B, Chatterjee T, et al. Renal Insufficiency Following Radiocontrast Exposure Trial (REINFORCE): a randomized comparison of sodium bicarbonate versus sodium chloride hydration for the prevention of contrast-induced nephropathy. Coron Artery Dis. 2008;19(6):413-9.
- Akyuz S, Karaca M, Kemaloglu Oz T, et al. Efficacy of oral hydration in the prevention of contrast-induced acute kidney injury in patients undergoing coronary angiography or intervention. Nephron Clin Pract. 2014;128(1-2):95-100.
- Barbanti M, Gulino S, Capranzano P, et al. Acute kidney injury with the renalguard system in patients undergoing transcatheter aortic valve replacement. JACC Cardiovasc Interv. 2015 Oct;8(12):1595-604.
- Boucek P, Havrdova T, Oliyarnyk O, et al. Prevention of contrast-induced nephropathy in diabetic patients with impaired renal function: a randomized, double blind trial of sodium bicarbonate versus sodium chloride-based hydration. Diabetes Res Clin Pract. 2013;101(3):303-8.
- Brar SS, Aharonian V, Mansukhani P, et al. Haemodynamic-guided fluid administration for the prevention of contrast-induced acute kidney injury: the POSEIDON randomised controlled trial. Lancet. 2014;383(9931):1814-23.
- Brar SS, Shen AY, Jorgensen MB, et al. Sodium bicarbonate vs sodium chloride for the prevention of contrast mediuminduced nephropathy in patients undergoing coronary angiography: a randomized trial. JAMA. 2008;300(9):1038-46.
- Briguori C, Visconti G, Focaccio A, et al. Renal Insufficiency After Contrast Media Administration Trial II (REMEDIAL II) RenalGuard system in high-risk patients for contrast-induced acute kidney injury. Circulation. 2011;124(11):1260-9.
- Briguori C, Airoldi F, D'Andrea D, et al. Renal insufficiency following contrast media administration trial (REMEDIAL) a randomized comparison of 3 preventive strategies. Circulation. 2007;115(10):1211-7.
- Burgess WP, Walker PJ. Mechanisms of contrast-induced nephropathy reduction for saline (NaCl) and sodium bicarbonate (NaHCO3). Biomed Res Int. 2014.
- Castini D, Lucreziotti S, Bosotti L, et al. Prevention of Contrast-induced Nephropathy: A Single Center Randomized Study. Clin Cardiol. 2010;33(3):E63-8.
- Chen SL, Zhang J, Yei F, Et al. Clinical outcomes of contrast-induced nephropathy in patients undergoing percutaneous coronary intervention: a prospective, multicenter, randomized study to analyze the effect of hydration and acetylcysteine. Int J Cardiol. 2008 Jun 6;126(3):407-13.
- Cho R, Javed N, Traub D, et al. Oral Hydration and Alkalinization is Noninferior to Intravenous Therapy for Prevention of Contrast-Induced Nephropathy in Patients with Chronic Kidney Disease. J Intervent Cardiol. 2010;23(5):460-6.
- Chong E, Poh KK, Lu Q, Et al. Comparison of combination therapy of high-dose oral N-acetylcysteine and intravenous sodium bicarbonate hydration with individual therapies in the reduction of Contrast-induced Nephropathy during Cardiac Catheterisation and Percutaneous Coronary Intervention (CONTRAST): A multi-centre, randomised, controlled trial. Int J Cardiol. 2015 Dec 15;201:237-42.
- Dussol B, Morange S, Loundoun A, et al. A randomized trial of saline hydration to prevent contrast nephropathy in chronic renal failure patients. Nephrol Dial Transplant, 2006;21(8), 2120-2126.
- Gomes VO, Lasevitch R, Lima VC, et al. Hydration with sodium bicarbonate does not prevent contrast nephropathy: a multicenter clinical trial. Arq Bras Cardiol. 2012;99(6):1129-34.
- Hafiz AM, Jan MF, Mori N, et al. Prevention of contrast-induced acute kidney injury in patients with stable chronic renal disease undergoing elective percutaneous coronary and peripheral interventions: Randomized comparison of two preventive strategies. Cathet Cardiovasc Intervent. 2012;79(6):929-37.
- Jurado-Román A, Hernández-Hernández F, García-Tejada J, et al. Role of hydration in contrast-induced nephropathy in patients who underwent primary percutaneous coronary intervention. Am J Cardiol. 2015 May 1;115(9):1174-8.
- Klima T, Christ A, Marana I, et al. Sodium chloride vs. sodium bicarbonate for the prevention of contrast medium-induced nephropathy: a randomized controlled trial. Eur Heart J. 2012;33(16):2071-9.
- Koc F, Ozdemir K, Altunkas F, et al. Sodium bicarbonate versus isotonic saline for the prevention of contrast-induced nephropathy in patients with diabetes mellitus undergoing coronary angiography and/or intervention: a multicentre prospective randomized study. J Investig Med. 2013 Jun;61(5):872-7.
- Kong DG, Hou YF, Ma LL, et al. Comparison of oral and intravenous hydration strategies for the prevention of contrast-induced nephropathy in patients undergoing coronary angiography or angioplasty: a randomized clinical trial. Acta Cardiol. 2012;67(5), 565-569.
- Kooiman J, Sijpkens YW, van Buren M, et al. Randomised trial of no hydration vs. sodium bicarbonate hydration in patients with chronic kidney disease undergoing acute computed tomographypulmonary angiography. J Thromb Haemostasis. 2014;12(10):1658-66.
- Kooiman J, Sijpkens YW, de Vries JP, et al. A randomized comparison of 1-h sodium bicarbonate hydration versus standard peri-procedural saline hydration in patients with chronic kidney disease undergoing intravenous contrast-enhanced computerized tomography. Nephrol Dial Transplant. 2014;29(5):1029-36.
- Lawlor DK, Moist L, DeRose G, et al. Prevention of contrast-induced nephropathy in vascular surgery patients. Ann Vasc Surg. 2007 Sep;21(5):593-7.
- Lee SW, Kim WJ, Kim YH, et al. Preventive strategies of renal insufficiency in patients with diabetes undergoing intervention or arteriography (the PREVENT Trial). Am J Cardiol. 2011;107(10):1447-52.
- Luo Y, Wang X, Ye Z, et al. Remedial hydration reduces the incidence of contrast-induced nephropathy and short-term adverse events in patients with ST-segment elevation myocardial infarction: a single-center, randomized trial. Intern Med. 2014;53(20):2265-72.
- Maioli M, Toso A, Leoncini M, et al. Sodium bicarbonate versus saline for the prevention of contrast-induced nephropathy in patients with renal dysfunction undergoing coronary angiography or intervention. J Am Coll Cardiol. 2008;52(8):599-604.
- Maioli M, Toso A, Leoncini M, et al. Effects of hydration in contrast-induced acute kidney injury after primary angioplasty: a randomized, controlled trial. Circ Cardiovasc Interv. 2011 Oct 1;4(5):456-62.
- Manari A, Magnavacchi P, Puggioni E, et al. Acute kidney injury after primary angioplasty: effect of different hydration treatments. J Cardiovasc Med.. 2014;15(1):60-7.
- Marenzi G, Ferrari C, Marana I, et al. Prevention of contrast nephropathy by furosemide with matched hydration: the MYTHOS (induced diuresis with matched hydration compared to standard hydration for contrast induced nephropathy prevention) trial. JACC Cardiovasc Intervent. 2012;5(1):90-7.
- Martin-Moreno PL, Varo N, Martínez-Ansó E, et al. Comparison of intravenous and oral hydration in the prevention of contrast-induced acute kidney injury in low-risk patients: a randomized trial. Nephron. 2015;131(1):51-8.
- Masuda M, Yamada T, Mine T, et al. Comparison of usefulness of sodium bicarbonate versus sodium chloride to prevent contrast-induced nephropathy in patients undergoing an emergent coronary procedure. Am J Cardiol. 2007;100(5), 781-786.
- Merten GJ, Burgess WP, Gray LV, et al. Prevention of contrast-induced nephropathy with sodium bicarbonate: a randomized controlled trial. JAMA; 2004; 2328-2334.
- Motohiro M, Kamihata H, Tsujimoto S, et al. A new protocol using sodium bicarbonate for the prevention of contrast-induced nephropathy in patients undergoing coronary angiography. Am J Cardiol. 2011;107(11):1604-8.
- Nieto-Ríos JF, Salazar WA, Sánchez OM, et al. Prevention of contrast induced nephropathy with sodium bicarbonate (the PROMEC study). J Brasil Nefrolo. 2014;36(3):360-6.
- Nijssen EC, Rennenberg RJ, Nelemans PJ, et al. Prophylactic hydration to protect renal function from intravascular iodinated contrast material in patients at high risk of contrast-induced nephropathy (AMACING): a prospective, randomised, phase 3, controlled, open-label, non-inferiority trial. Lancet. 2017 Apr 1;389(10076):1312-1322.
- Ozcan EE, Guneri S, Akdeniz B, et al. Sodium bicarbonate, N-acetylcysteine, and saline for prevention of radiocontrast-induced nephropathy. A comparison of 3 regimens for protecting contrast-induced nephropathy in patients undergoing coronary procedures. A single-center prospective controlled trial. Am Heart J. 2007;154(3):539-44.
- Qian G, Fu Z, Guo J, et al. Prevention of contrast-induced nephropathy by central venous pressureguided fluid administration in chronic kidney disease and congestive heart failure patients. JACC Cardiovasc Intervent. 2016;9(1):89-96.
- Ratcliffe JA, Thiagarajah P, Chen J, et al. Prevention of contrast-induced nephropathy: A randomized controlled trial of sodium bicarbonate and N-acetylcysteine. Int J Angiol. 2009;18(4):193-7.
- Recio-Mayoral A, Chaparro M, Prado B, et al. The reno-protective effect of hydration with sodium bicarbonate plus N-acetylcysteine in patients undergoing emergency percutaneous coronary intervention: the RENO Study. J Am Coll Cardiol. 2007;49(12):1283-8.
- Shavit L, Korenfeld R, Lifschitz M, et al. Sodium bicarbonate versus sodium chloride and oral N-acetylcysteine for the prevention of contrast-induced nephropathy in advanced chronic kidney disease. J Intervent Cardiol. 2009;22(6):556-63.
- Solomon R, Gordon P, Manoukian SV, et al. Randomized trial of bicarbonate or saline study for the prevention of contrast-induced nephropathy in patients with CKD. Clin J Am Soc Nephrol, 2015;10(9), 1519-1524.
- Tamura A, Goto Y, Miyamoto K, et al. Efficacy of single-bolus administration of sodium bicarbonate to prevent contrast-induced nephropathy in patients with mild renal insufficiency undergoing an elective coronary procedure. Am J Cardiol. 2009;104(7):921-5.
- Taylor AJ, Hotchkiss D, Morse RW, et al. PREPARED: Preparation for Angiography in Renal Dysfunction: a randomized trial of inpatient vs outpatient hydration protocols for cardiac catheterization in mild-to-moderate renal dysfunction. Chest. 1998 Dec;114(6):1570-4.
- Trivedi HS, Moore H, Nasr S, et al. A randomized prospective trial to assess the role of saline hydration on the development of contrast nephrotoxicity. Nephron Clin Pract. 2003 Jan;93(1):C29-34.
- Ueda H, Yamada T, Masuda M, et al. Prevention of contrast-induced nephropathy by bolus injection of sodium bicarbonate in patients with chronic kidney disease undergoing emergent coronary procedures. Am J Cardiol. 2011;107(8):1163-7.
- Usmiani T, Andreis A, Budano C, et al. AKIGUARD (Acute Kidney Injury GUARding Device) trial: in-hospital and one-year outcomes. medicine Cardiovasc Med (Hagerstown, Md.). 2016;17(7):530-7.
- Visconti G, Focaccio A, Donahue M, et al. RenalGuard System for the prevention of acute kidney injury in patients undergoing transcatheter aortic valve implantation. EuroIntervention. 2016 Apr 8;11(14):e1658-61.
- Wróbel W, Sinkiewicz W, Gordon M, et al. Oral versus intravenous hydration and renal function in diabetic patients undergoing percutaneous coronary interventions. Kardiol Pol. 2010 Sep;68(9):1015-20.
Evidence tabellen
Table: Exclusion after revision of full text
|
Author and year |
Reason for exclusion |
|
Akyuz. 2014 |
Patients with normal kidney function |
|
Alessandri, 2014 |
Patients with normal kidney function |
|
Cho, 2010 |
Does not fulfill selection criteria |
|
Heguilen, 2013 |
Not using the most widely used PC-AKI definition of SC rise ≥25% or 44µmol/l |
|
Koc, 2013 |
Patients with normal kidney function |
|
Kong, 2012 |
Patients with normal kidney function |
|
Kotlyar, 2005 |
Does not fulfill inclusion criteria (compares iv hydration with N-acetylcysteïne to hydration with placebo, not different hydration strategies) |
|
Lawlor, 2007 |
Mixture of oral and intravenous hydration, compared to intravenous hydration alone |
|
Mahmoodi, 2014 |
Patients with normal kidney function |
|
Manari, 2014 |
The studied hydration infusion mixture is not used in Dutch clinical practice |
|
Martin-Moreno, 2015 |
Patients with normal kidney function |
|
Mueler, 2005 |
Does not fulfill inclusion criteria (no control group) |
|
Pakfetrat, 2009 |
The studied hydration infusion mixture is not used in Dutch clinical practice |
|
Taylor, 1998 |
Mixture of oral and intravenous hydration, compared to intravenous hydration alone |
|
Thayssen, 2014 |
Patients with normal kidney function |
|
Trivedi, 2003 |
Normal kidney function |
|
Vashegani Ferahani, 2009 |
The studied hydration infusion mixture is not used in Dutch clinical practice |
|
Wrobel, 2014 |
Did not define CIN/CI-AKI/PC-AKI |
|
Yeghanehkah, 2014 |
The studied hydration infusion mixture is not used in Dutch clinical practice |
Table 1 Adverse events in bicarbonate versus saline infusion or controlled hydration versus standard hydration.
|
Author and date |
Mortality |
Dialysis |
Heart failure or edema |
|||
|
|
Bicarbonate |
Saline |
Bicarbonate |
Saline |
Bicarbonate |
Saline |
|
Patients recieving short schedules of hydration with either bicarbonate or saline for CAG/PCI |
||||||
|
Adolph, 2008 |
NR |
NR |
0/71 |
0/74 |
NR |
NR |
|
Boucek, 2013 |
0/51 |
0/49 |
1/51 |
2/49 |
NR |
NR |
|
Brar, 2008 |
4/175 |
7/178 |
2/175 |
4/178 |
NR |
NR |
|
Gomes, 2012 |
6/150 |
7/151 |
NR |
NR |
NR |
NR |
|
Masuda, 2004 |
NR |
NR |
NR |
NR |
NR |
NR |
|
Merten, 2004 |
0/30 |
2/29 |
1/30 |
3/29 |
11/30 |
11/29 |
|
Ozcan, 2007 |
NR |
NR |
1/88 |
1/88 |
0/88 |
0/88 |
|
Ratcliffe, 2009 |
0/42 |
0/36 |
0/42 |
0/36 |
0/42 |
0/36 |
|
Recio-Mayoral, 2007 |
1/180 |
4/188 |
1/180 |
3/186 |
1/180 |
2/188 |
|
Solomon, 2015 |
|
|
|
|
|
|
|
Total |
11/658 |
20/631 |
6/637 |
13/640 |
12/340 |
13/341 |
|
Patients recieving short schedules for bicarbonate versus long schedule for saline for CAG/PCI |
||||||
|
Briguori, 2007 |
NR |
NR |
1/108 |
1/111 |
NR |
NR |
|
Castini, 2010 |
NR |
NR |
0/52 |
0/51 |
NR |
NR |
|
Hafiz, 2012 |
0/159 |
0/151 |
0/159 |
0/151 |
0/159 |
0/151 |
|
Klima, 2011 |
0/169 |
0/89 |
0/169 |
0/89 |
0/169 |
0/89 |
|
Koc, 2013 |
NR |
NR |
NR |
NR |
NR |
NR |
|
Lee, 2011 |
6/193 |
2/189 |
10/193 |
3/189 |
0/193 |
0/189 |
|
Maioli, 2008 |
4/250 |
3/252 |
1/250 |
1/252 |
NR |
NR |
|
Nieto-Rios, 2014 |
NR |
NR |
NR |
NR |
8/103 |
7/113 |
|
Shavit, 2009 |
NR |
NR |
0/51 |
0/36 |
NR |
NR |
|
Total |
12/927 |
5/838 |
12/982 |
5/879 |
8/624 |
7/542 |
|
Patients recieving bicarbonate or saline hydration in “other” hydration schemes for coronary angiography |
||||||
|
Chong, 2015 |
NR |
NR |
0/157 |
1/153 |
NR |
NR |
|
Motohiro, 2011 |
NR |
NR |
0/78 |
0/77 |
0/78 |
0/77 |
|
Tamuro, 2009 |
NR |
NR |
0/72 |
1/72 |
0/72 |
0/72 |
|
Ueda, 2011 |
2/30 |
3/29 |
0/30 |
0/29 |
0/30 |
0/29 |
|
Patients receiving controlled hydration |
||||||
|
|
C.H. |
Control |
C.H. |
Control |
C.H. |
Control |
|
Barbanti, 2015 |
1/56 |
2/56 |
0/56 |
0/56 |
NR |
NR |
|
Brar, 2014 |
1/196 |
4/200 |
1/196 |
8/200 |
NR |
NR |
|
Briguori, 2011 |
NR |
NR |
1/146 |
6/146 |
NR |
NR |
|
Marenzi, 2012 |
1/87 |
2/83 |
1/87 |
3/93 |
5/87 |
10/83 |
|
Qian, 2016 |
4/134 |
13/135 |
NR |
NR |
5/134 |
4/135 |
|
Usmiani, 2016 |
4/59 |
8/65 |
0/59 |
2/65 |
NR |
NR |
|
Visconti, 2016 |
NR |
NR |
0/22 |
2/26 |
NR |
NR |
|
Totaal |
11/532 |
29/539 |
3/566 |
21/586 |
10/221 |
14/218 |
C.H.: controlled hydration; NR: not reported
Research question
|
Study reference
(first author, publication year) |
Describe method of randomisation1 |
Bias due to inadequate concealment of allocation?2
(unlikely/likely/unclear) |
Bias due to inadequate blinding of participants to treatment allocation?3
(unlikely/likely/unclear) |
Bias due to inadequate blinding of care providers to treatment allocation?3
(unlikely/likely/unclear) |
Bias due to inadequate blinding of outcome assessors to treatment allocation?3
(unlikely/likely/unclear) |
Bias due to selective outcome reporting on basis of the results?4
(unlikely/likely/unclear) |
Bias due to loss to follow-up?5
(unlikely/likely/unclear) |
Bias due to violation of intention to treat analysis?6
(unlikely/likely/unclear) |
|
|
Hydration versus no hydration |
|||||||||
|
Kooiman, 2014 |
Computer generated allocation sequence (stratified by hospital and renal function) |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
|
|
Nijssen, 2017 |
Computer- generated using ALEA screening and enrolment application software. |
Unlikely |
Likely |
Likely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
|
|
Oral hydration |
|||||||||
|
Cho, 2010 |
Not decribed: “randomly assigned” |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
Unclear |
|
|
Dussol, 2006 |
Computer generated randomization list |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
|
|
Sodium bicarbonate short schedule versus saline short schedule for coronary angiography and/or percutaneous intervention |
|||||||||
|
Adolph, 2008 |
Computer-generated randomization schedule |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
Unclear |
|
|
Boucek, 2013 |
Computer-generated randomization schedule with the use of numbered opaque envelopes containing identification of assigned medication |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
|
|
Brar, 2008 |
Computer-generated randomization schedule |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
|
|
Gomes, 2012 |
Not decribed: “randomly assigned” |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
Unlikely |
|
|
Huber, 2016 |
Computer-generated randomization list |
Unlikelu |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
Unclear |
|
|
Manari, 2014 |
Computer generated balanced randomization list |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
Unclear |
|
|
Ozcan, 2007 |
Not decribed: “randomly assigned” |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
Unclear |
|
|
Ratcliffe, 2009 |
Not decribed: “randomization block” |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Likely |
Unclear |
|
|
Recio-Mayoral, 2007 |
Not decribed: “randomly assigned” |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
Unlikely |
|
|
Sodium bicarbonate short schedule versus saline long schedule for coronary angiography and/or percutaneous intervention |
|||||||||
|
Briguori, 2007 |
Computer-generated randomization schedule |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
|
|
Castini, 2008 |
Computer-generated randomization table |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
Unclear |
|
|
Hafiz, 2012 |
Random allocation table |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
|
|
Klima, 2012 |
Sealed envelopes |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
|
|
Lee, 2011 |
Interactive web response system, computer generated randomization, stratified by participating center |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
|
|
Maioli, 2008 |
Computerized open-label assignment in blinded envelopes used in a consecutive fashion |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
|
|
Nieto-Rios, 2014 |
Sealed opaque envelopes (random numbers table) |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
|
|
Shavit, 2009 |
Not described |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
|
|
Sodium bicarbonate versus saline: “other schedules” for coronary angiography and/or percutaneous intervention |
|||||||||
|
Chong, 2015 |
Block randomisation, stratified by site, using aweb-randomisation system or back-up randomisation envelopes. |
Unlikely |
Likely |
Unclear |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
|
|
Motohiro, 2011 |
Computer-generated random numbers |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
|
|
Tamura, 2009 |
Computer-generated random numbers |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
|
|
Turedi, 2016 |
Computer-based block randomization. |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
Unlikely |
|
|
Ueda, 2011 |
Computer-generated random numbers |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
|
|
Sodium bicarbonate short schedule versus saline long schedule for computed tomography |
|||||||||
|
Kooiman, 2014 |
Computer-generated allocation sequence |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
|
|
Controlled diuresis |
|||||||||
|
Brar, 2014 |
Computer-generated concealed randomisation schedule |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
|
|
Barbanti, 2015 |
Randomization based on computer generated codes |
Unlikely |
Likely |
Likely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
|
|
Briguori, 2011 |
Computer-generated randomisation list |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
|
|
Marenzi, 2012 |
Computer-generated random numbers |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
|
|
Qian, 2016 |
“randomly assigned” |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
|
|
Usmiani, 2015 |
“randomly assigned” |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unlikely |
Unclear |
|
|
Usmiani, 2016 |
Randomly subdivided |
Unlikely |
Likely |
Likely |
Unlikely |
Unlikely |
Unclear |
Unlikely |
|
|
Visconti, 2016 |
Prospective, non-randomised study |
Likely |
Unclear |
Unclear |
Unclear |
Unlikely |
Unclear |
Unclear |
|
1. Randomisation: generation of allocation sequences have to be unpredictable, for example computer generated random-numbers or drawing lots or envelopes. Examples of inadequate procedures are generation of allocation sequences by alternation, according to case record number, date of birth or date of admission.
- Allocation concealment: refers to the protection (blinding) of the randomisation process. Concealment of allocation sequences is adequate if patients and enrolling investigators cannot foresee assignment, for example central randomisation (performed at a site remote from trial location) or sequentially numbered, sealed, opaque envelopes. Inadequate procedures are all procedures based on inadequate randomisation procedures or open allocation schedules..
- Blinding: neither the patient nor the care provider (attending physician) knows which patient is getting the special treatment. Blinding is sometimes impossible, for example when comparing surgical with non-surgical treatments. The outcome assessor records the study results. Blinding of those assessing outcomes prevents that the knowledge of patient assignement influences the proces of outcome assessment (detection or information bias). If a study has hard (objective) outcome measures, like death, blinding of outcome assessment is not necessary. If a study has “soft” (subjective) outcome measures, like the assessment of an X-ray, blinding of outcome assessment is necessary.
- Results of all predefined outcome measures should be reported; if the protocol is available, then outcomes in the protocol and published report can be compared; if not, then outcomes listed in the methods section of an article can be compared with those whose results are reported.
- If the percentage of patients lost to follow-up is large, or differs between treatment groups, or the reasons for loss to follow-up differ between treatment groups, bias is likely. If the number of patients lost to follow-up, or the reasons why, are not reported, the risk of bias is unclear
- Participants included in the analysis are exactly those who were randomized into the trial. If the numbers randomized into each intervention group are not clearly reported, the risk of bias is unclear; an ITT analysis implies that (a) participants are kept in the intervention groups to which they were randomized, regardless of the intervention they actually received, (b) outcome data are measured on all participants, and (c) all randomized participants are included in the analysis.
Evidence table for intervention studies (randomized controlled trials and non-randomized observational studies [cohort studies, case-control studies, case series])1
This table is also suitable for diagnostic studies (screening studies) that compare the effectiveness of two or more tests. This only applies if the test is included as part of a test-and-treat strategy – otherwise the evidence table for studies of diagnostic test accuracy should be used.
Research question
|
Study reference |
Study characteristics |
Patient characteristics 2 |
Intervention (I) |
Comparison / control (C) 3
|
Follow-up |
Outcome measures and effect size 4 |
Comments |
|
Hydration versus no hydration |
|||||||
|
Kooiman, 2014 |
Type of study: randomized controlled trial
Setting: emergency patients, multiple centers, both in- and outpatients
Country: the Netherlands
Source of funding: non-commercial |
Inclusion criteria: 1) adult patients ≥18 years with a clinical suspicion of a pulmonary embolis requiring computed tomography-pulmonary angiography (CTPA) 2) chronic kidney disease (CKD): eGFR <60mL/min/1.73m2
Exclusion criteria: 1) pregnancy 2) previous contrast administration within past 7 days 3) documented allergy for iodinated contrast media 4) hemodynamic instability (systolic blood pressure <100mmHg) 5) earlier participation in samen trial
N total at baseline: Intervention: 67 Control: 71
Important prognostic factors2: For example age ± SD: I: 70 ± 12 C: 71 ± 13
Sex: I: 52% M C: 48% M
eGFR ± SD: I: 50 ± 16 C: 48 ± 15
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
Withholding hydration prior to CTPA
|
Describe control (treatment/procedure/test):
250mL iv 1.4% sodium bicarbonate 1 hour before CTPA |
Length of follow-up: 96 hours
Loss-to-follow-up: 3/138 (2.2%) 2 lost to follow-up 1 died
Incomplete outcome data: As above
|
Outcome measures and effect size (include 95%CI and p-value if available):
CI-AKI (= creatinine increase >25% / >0.5mg/dL) I: 6 (9%) C: 5 (7%) RR: 1.29, 95% CI: 0.41 – 4.03
None of the patients developed a need for dialysis |
Authors’ conclusion:
Our results suggest that preventive hydration could be safely withheld in CKD patients undergoing CTPA for suspected acute pulmonary embolism. |
|
Nijssen, 2017 (AMACING) |
Type of study: randomized controlled trial
Setting: elective patients, one university hospital
Country: the Netherlands
Source of funding: Stichting de Weijerhorst |
Inclusion criteria: 1) eGFR: 45-59 mL/min/1.73m2 combined with either diabetes, or at least two predefined risk factors (age>75y; anaemia defined as haematocrit values <0.39L/L for men, and <0.36L/L for women; cardiovascular disease; non-steroidal anti-inflammatory drug; or diuretic nephrotoxic medication).
Exclusion criteria: 1) Inability to obtain informed consent; 2) eGFR lower than 30mL per min/1.73m2; 3) renal replacement therapy; 4)emergency procedures; 5) intensive care patients; 6) known inability to perform primary endpoint data collection; 7) no referral to prophylactic hydration; 8) participation in other RCT; and 9) isolation due to infection control
N total at baseline: Intervention: 328 (I1: 328, I2: 296) Control: 332 (C1: 332, C2: 307)
Important prognostic factors2: For example age ± SD: I: 71.9 ± 9.3 C: 72.6 ± 9.3
Sex: I: 59% M C: 64% M
Baseline SCr: I:118.7±28μmol/L C:117.7±25μmol/L
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
Prophylactic hydration protocols according to current guidelines:
Standard protocol intravenous 0.9% NaCl 3–4 mL/kg per h during 4 h before and 4 h after contrast administration; long protocol intravenous 0.9% NaCl 1 mL/kg per h during 12 h before and 12 h after contrast administration. |
Describe control (treatment/procedure/test):
No prophylactic treatment. |
Length of follow-up: 2-6 days
Loss-to-follow-up: I: 68/328 C: 25/332
Incomplete outcome data: As above
|
Outcome measures and effect size (include 95%CI and p-value if available):
CI-AKI (25% or 44 μmol/L within 2–6 days of contrast exposure) I:8 (2.7%) C: 8 (2.6%) P=0.417
No hydration was cost-saving relative to hydration.
No haemodialysis or related deaths occurred within 35 days. |
Authors’ conclusion:
‘We found no prophylaxis to be non-inferior and cost-saving in preventing contrast-induced nephropathy compared with intravenous hydration according to current clinical practice guidelines.’ |
|
Oral hydration |
|||||||
|
Cho, 2010 |
Type of study: randomized controlled trial
Setting: elective patients, one hospital
Country: United States of America
Source of funding: not reported |
Inclusion criteria: 1) patients 18 years or older with stable serum creatinine levels of at least 1.1mg/dL or estimated creatinine clearance less than 60mL/min scheduled for diagnostic, elective angiography
Exclusion criteria: 1) serum creatinine levels >8.0mg/dL 2) change in serum creatinine levels of at least 0.5mg/dL during the previous 24 hours 3) pre-existing dialysis 4) multiple myeloma or other myeloproliferative disease 5) current decompensated heart failure or significant change in NYHA 6) current myocardial infarction 7) symptomatic hypokalaemia 8) uncontrolled hypertension 9) exposure to radiocontrast within 7 days of enrolment into this study 10) emergency catheterisation 11) allergy to radiographic contrast 12) pregnancy 13) administration of mannitol, feoldapam or NAC during the time of the study 14) exacerbation of chronic obstructive pulmonary disease 15) serum bicarbonate greater than 28eEw/L and sodium less than 133mEq/L
N total at baseline: Intervention: 43 (I1: 22, I2: 22) Control: 48 (C1: 27, C2: 21)
Important prognostic factors2: For example age ± SD: I1: 81 ± 7 I2: 79 ± 2 C1: 77 ± 8 C2: 78 ± 9
Sex: I1: 45% M I2: 38% M C1: 63% M C2: 52
Baseline SCr: I1: 1.38 I2: 1.31 C1: 1.38 C2: 1.41
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
1) oral hydration with 500mL of water to be started 4 hours prior to contrast exposure and stopped 2 hours prior to procedure followed by oral hydration with 600mL water postprocedure
2) oral hydration with 500mL of water to be started 4 hours prior to procedure and stopped 2 hours prior to contrast exposure, with the addition of 3.9g (46.4mEq) of oral sodium bicarbonate to be given 20 minutes prior to contrast exposure followed by oral hydration with 600mL of water and 1.95g (30.4mEq) of oral sodium bicarbonate 2 hours and 4 hours after the initial dose
|
Describe control (treatment/procedure/test):
1) pretreatment with a 3mL/kg bolus of intravenous saline solution (154mEq/L) over 1 hour priori to contrast exposure Intravenous infusion of 1mL/kg for 6 hours after procedure
2) pretreatment with a 3mL/kg bolus of intravenous sodium biacrbonate solution (154mEq/L) over 1 hour priori to contrast exposure Intravenous infusion of 1mL/kg for 6 hours after procedure
|
Length of follow-up: 72 hours
Loss-to-follow-up: Not reported
Incomplete outcome data: Not reported
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN (= >25% increase in sCr from baseline or an absolute increase of 0.5mg/dL from baseline at 72 hours following exposure to radio-contrast) I1: 1/22 I2: 1/22 C1: 6/27 C2: 2/21 p>0.05
There were no in-hospital mortalities during this study.
Length of hospital stay did not differ significantly between groups. |
Authors’ hydration:
Oral hydration with or without sodium bicarbonate prior to and following CAG is not inferioir to intravenous hydration and sodium bicarbonate with respect to CIN; and to date, offers an equivalent and practical approach in preventing a decline in renal functionafter contrast exposure without accuring additional delay in hospital days or in-hospital mortality, |
|
Dussol, 2006 |
Type of study: randomized controlled trial
Setting: elective patients, one university hospital
Country: France
Source of funding: non-commercial |
Inclusion criteria: 1) patients referred for any radiological procedures necessitating a contrast medium injection and who had a baseline Cockcroft clearance between 15-60ml/min 2) either chronic renal failure and on a kidney graft
Exclusion criteria: 1) <18 years old 2) women of child-bearing age not using contraception or breast feeding 3) patients with heart failure and ejection fraction <30% 4) uncontrolled arterial hypertension 5) obvious extracellular overhydration 6) respiratory depression 7) known prior intolerance to theophylline or furosemide 8) previous exposure to contrast media in the 14 days before randomization 9) unwilling or unable to provide informed consent 10) adequate time prior to contrast media injection was not available to perform the study procedure 11) if sCr measurements varied by >10% in the previous weeks before referral
N total at baseline: Intervention: Control:
Important prognostic factors2: For example age ± SD: I: 63 ± 15 C: 64 ± 11
Sex: I: 66% M C:75 % M
eGFR ± SD: I: 38 ± 13 C: 33 ± 11
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
NaCl 1g/10kg/day per os for 2 days
|
Describe control (treatment/procedure/test):
0.9% saline iv 15ml/kg for 6 hours before the procedure |
Length of follow-up: 48 hours
Loss-to-follow-up: Not reported per group separately, in total 3/315 (1%) lost to follow-up
Incomplete outcome data: As above
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN (= increase in the baseline sCr concentration of at least 44µmol/L (0.5mg/dL) within 48 hours after the injection of contrast media) I: 5/76 (7%) C: 4/77 (5%) p>0.05
None of the patients had fluid overload |
Authors’ conclusion:
Oral saline hydration was as efficient as intravenous saline hydration for the prevention of CIN in patients with stage 3 renal diseases. |
|
Sodium bicarbonate short schedule versus saline short schedule for coronary angiography and/or percutaneous intervention |
|||||||
|
Adolph, 2008 |
Type of study: randomized controlled trial
Setting: elective patients
Country: Germany
Source of funding: not reported |
Inclusion criteria: 1) patients >18 years with baseline serum creatinine concentration greater than 106µmol/L (1.2mg/dL) undergoing elective diagnostic or interventional coronary angiography
Exclusion criteria: 1) acute myocardial infarction 2) allergies to trial medication 3) exposure to contrast mediumwithin the last 7 days 4) thyroid dysfunction 5) pregnancy 6) uncontrolled hypertension 7) life-limiting concomitant disease 8) pulmonary edema 9) chronic dialysis 10) administration of dopamine, mannitol, fenoldopam or NAC during the study
N total at baseline: Intervention: 71 Control: 74
Important prognostic factors2: For example age ± SD: I: 70 ± 8 C: 73 ± 7
Sex: I: 75% M C: 81% M
sCr (mg/dL ± SD) I: 1.54 ± 0.51 C: 1.57 ± 0.36
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
Sodium bicarbonate 154mEq/L in 5% dextrose solution 2ml/kg body weight/hour for 2 hours before And 1ml/kg body weight/hour during and for 6 hours after contrast administration
|
Describe control (treatment/procedure/test):
Sodium chloride 154 mEq/L in 5% dextrose solution 2ml/kg body weight/hour for 2 hours before And 1ml/kg body weight/hour during and for 6 hours after contrast administration
|
Length of follow-up: 2 days
Loss-to-follow-up: 1 patient (refused follow-up)
Incomplete outcome data: 3/145 (2%) 2 patients had an emergency coronary bypass and pulmonary edema 1 patient refused follow-up
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN (= elevation of sCr concentration >0.5mg/dL (44µmol/L) or 25%above baseline between day 0 and days 1 or 2 after contrast axposure) I: 4.2% C: 2.7% P=0.61
Dialysis for acute renal failure was not required |
Authors’ conclusion:
Renal Insufficiency following radiocontrast exposure demonstrates a homogenously low rate of CIN after exposure to non-ionic, iso-osmolar iodixanol regardless of the use of either bicarbonate sodium or sodium chloride solution for volume supplementation. |
|
Boucek, 2013 |
Type of study: RCT
Setting: elective inpatients, one hospital
Country: Czech Republic
Source of funding: commercial |
Inclusion criteria: 1) presence of diabetes mellitus 2) renal function impairment (screening serum creatinine _100 mmol/L), 3) age of ≥18 years 4) a planned procedure with intra-arterial or intravenous use of contrast
Exclusion criteria: 1) endstage renal disease (screening serum creatinine _500 mmol/L, 2) chronic dialysis treatment or presence of kidney transplant), 3) pre-planned dialysis following the contrast-involving procedure, 4) emergency type of procedure, acute kidney injury (serum creatinine increase _50 mmol/L during the previous 24-h period), 5) volume overload with left ventricular failure, 6) uncontrolled hypertension (systolic BP _180 or diastolic BP _110 mmHg), 7) hemodynamic instability (systolic BP <90 and diastolic BP <50 mmHg), 8) contrast use in the previous 48-h period, 9) multiple myeloma, 10) pregnancy or breastfeeding 11) pre-planned use of any other measure for CIN prevention apart from the NaCl or NaHCO3 infusions
N total at baseline: Intervention: 61 Control: 59
Important prognostic factors2: For example age ± SD: I: 63 ± 11 C: 67 ± 10
Sex: I: 75% M C: 75% M
eGFR (mL/min/1.73m2) ± SD I: 44 ± 19 C: 25 ± 17
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
1.4% sodium bicarbonate in 5% glucose 3ml/kg/hour 1 hour before contrast administration (limited to a maximum of 330mL) 1mL/kg/hour 6 hours after contrast administration (limited to a maximum of 660mL)
|
Describe control (treatment/procedure/test):
0.9% saline in 5% glucose 3ml/kg/hour 1 hour before contrast administration (limited to a maximum of 330mL) 1mL/kg/hour 6 hours after contrast administration (limited to a maximum of 660mL)
|
Length of follow-up: 2 days – laboratory parameters 1 month – clinical parameters
Loss-to-follow-up: Intervention: 3/61 (5%) Reasons not described
Control: 3/59 (5%) Reasons not described
Incomplete outcome data: As above
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN (= sCr increase of ≥25% and/or 44µmol/L (0.5mg/dL) within 2 days foillowing administration of contrast) I: 7 (12%) C: 5 (9%) P=0.76 Incidence rate ratio: 1.35 (95% CI: 0.37 – 5.41)
No patients died or experienced severe kidney injury with need for acute dialysis treatment. |
Authors’ conclusion:
In diabetic patients with renal function impairment sodium bicarbonate does not confer protection against contrast-induced nephropathy greater than sodium chloridebased hydration.
|
|
Brar, 2008 |
Type of study: randomized controlled trial
Setting: elective patients, one hospital
Country: United States of America
Source of funding: commercial |
Inclusion criteria: 1) an estimated glomerular filtration rate (GFR) of 60 mL/min per 1.73m2 or less, 2) age 18 years or older, 3) at least 1 of the follwing: -diabetes mellitus, -history of congestive heart failure, -hypertension (140/90 mm Hg treatment with an antihypertensive medication), -age older than 75 years
Exclusion criteria: 1) inability to obtain consent, 2) receipt of a sodium bicarbonate infusion prior to randomization, 3) emergency cardiac catheterization, 4) intra-aortic balloon counterpulsation, 5) dialysis, 6) exposure to radiographic contrast media within the preceding 2 days, 7) allergy to radiographic contrast media, 8) acutely decompensated congestive heart failure, 9) severe valvular abnormality (eg, severe aortic stenosis or mitral regurgitation), 10) single functioning kidney, 11) history of kidney or heart transplantation, 12) change in estimated GFR of 7.5% or more per day or a cumulative change of15%or more over the prior 2 or more days
N total at baseline: Intervention: 175 Control: 178
Important prognostic factors2: For example age (IQR range) I: 71 (65-75) C: 71 (65-76)
Sex: I: 65% M C: 62% M
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
1.4% sodium bicarbonate iv infusion Infusion was begun 1 hour prior to the start of contrast administration at3mL/kg for1hour, decreased to 1.5 mL/kg per hour during the procedure and for 4 hours following completion of theprocedure.Forpatientsweighing more than 100 kg, the bolus and infusion rate were limited to those used for patients weighing100kg
|
Describe control (treatment/procedure/test):
0.9% saline iv infusion Infusion was begun 1 hour prior to the start of contrast administration at3mL/kg for1hour, decreased to 1.5 mL/kg per hour during the procedure and for 4 hours following completion of theprocedure.Forpatientsweighing more than 100 kg, the bolus and infusion rate were limited to those used for patients weighing100kg |
Length of follow-up: 2-3 days for laboratory parameters 6 months for clinical effects
Loss-to-follow-up: Intervention: 17 (10%) Excluded 1 Did not undergo coronary angiography 16 Did not have estimated GFR data 1-4 d after procedure
Control: 13 (7%) Excluded 2 Did not undergo coronary angiography 11 Did not have estimated GFR data 1-4 d after procedure
Incomplete outcome data: As above for laboratory paramters. All patients were followed up for clinical events.
|
Outcome measures and effect size (include 95%CI and p-value if available):
I: 21/158 (13% C: 24/165 (15%) Absolute difference: 1.3, 95% CI: -6.3 to 8.8, p=0.75
Serum creatinine >25% or >0.5mg/dL increase I: 26/158 (17%) C: 30/165 (18%) Absolute difference: 1.7, 95% CI: -6.5 to 10.0, p=0.78
30-day mortality I: 3/175 (2%) C: 3/178 (2%) p>0.05
6-month mortality I: 34% C: 2% P=0.54
6-month start of dialysis I: 2/175 (1%) C: 4/178 (2%) P-value not reported
|
Authors’ conclusion:
The results of this study do not suggest that hydration with sodium bicarbonate is superior to hydration with sodium chloride for the prevention of contrast medium–induced nephropathy in patients with moderate to severe chronic kidney disease who are undergoing coronary angiography. |
|
Gomes, 2012 |
Type of study: randomized controlled trial
Setting: elective patients, 6 difference centres
Country: Brazil
Source of funding: none reported |
Inclusion criteria: 1) patients at moderate to high risk for developing CIN who were referred for elective coronary angiography or PCI at 6 centers 2) serum creatinine ≥ 1.2 mg/dL or glomerular filtration rate (GFR) <50 mL/min
Exclusion criteria: 1) age <18 years, 2) use of radiographic contrast media during the last 21 days, 3) history of dialysis, 4) cardiac insufficiency class III-IV NYHA, 5) emergency procedures
N total at baseline: Intervention: 150 Control: 151
Important prognostic factors2: For example age ± SD: I: 64 ± 12 C: 65 ± 12
Sex: I: 69% M C: 75% M
eGFR ± SD I: 51 ± 13 C: 52 ± 13
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
154 mEq/l of sodium bicarbonate in 5% dextrose and H2O 3 mL/ kg/ h for 1 hour immediately before contrast injection same fluid at a rate of 1 mL/kg/h during contrast exposure and for 6 hours after the procedure |
Describe control (treatment/procedure/test):
0.9% saline infusion 3 mL/ kg/ h for 1 hour immediately before contrast injection same fluid at a rate of 1 mL/kg/h during contrast exposure and for 6 hours after the procedure |
Length of follow-up: 48 hours
Loss-to-follow-up: Not reported
Incomplete outcome data: Not reported
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN (=an increase in serum creatinine ≥ 0.5 mg/dL 48 hours after exposure to contrast medium) I: 9/150 (6%) C: 9/151 (6%) P=0.97
Dialysis: I: 0% C: 0% P=1.00
Death: I: 3% C: 5% P=0.81 |
Authors’ conclusion:
Hydration with sodium bicarbonate was not superior to saline to prevent contrast media induced nephropathy in patients at risk undergoing cardiac catheterization. |
|
Huber, 2016 |
Type of study: randomized controlled
Setting: single-center university hospital
Country: Germany
Source of funding: institutional support |
Inclusion criteria: 1) >18 years; 2) increased risk of CIN undergoing administration of CM. High risk was defined by a serum creatinine level ≥1.1 or ≥0.8 mg/dL plus an additional risk factor like diabetes mellitus, renal failure in past medical history, or nephrotoxic medication (aminoglycoside, vancomycin, amphotericin B, and diuretic).
Exclusion criteria: 1) pre-existing renal replacement therapy; 2) unstable serum creatinine levels (difference of more than _0.4 mg/dL within 3 days before contrast application); 3) contraindi-cations for theophylline or sodium bicarbonate (allergies, tachycardia, alkalosis, and hypokalemia); and; 4) additional interventions that might influence renal function.
Important prognostic factors2: For example age ± SD: I: 64.4 ± 15.7 C: 66.1 ±13.3
Sex: I: 59.5% M C: 66.7% M
Baseline SCr: I:1.25± 0.69 mg/dL C:1.38± 0.65 mg/dL
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
Group B received bicarbonate infusion with 200mg theophylline.
|
Describe control (treatment/procedure/test):
Control group S received sodium chloride infusion with 200mg theophylline. |
Length of follow-up: 48h after CM
Loss-to-follow-up: I:14/91 C: 14/94
Incomplete outcome data: Not reported
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN as a raise in serum creatinine of _25% or _0.5 mg/dL within 48 h after contrast application I: 1/74 (1.4%) C: 7/78 (9%) P=0.039
Dialysis: I: 9% C: 17% P=0.189
|
Authors’ conclusion:
‘In patients at increased risk of CIN receiving prophylactic theophylline, hydration with sodium bicarbonate reduces contrast-induced renal impairment compared to hydration with saline.’ |
|
Manari, 2014 |
Type of study: randomized controlled
Setting: emergency patients, multicentre trial
Country: Italy
Source of funding: not reported |
Inclusion criteria: 1) Patients with STEMI within 12 h from symptom onset referred for primary angioplasty 2) age at least 18 years 3) chest pain lasting for at least 30 min associated with STsegment elevation of 0.2mV or more in at least two contiguous leads or new left bundle-branch block
Exclusion criteria: 1) the concomitant detection of mechanical complications, 2) previous peritoneal or hemodialysis treatment, 3) the presence of postanoxic coma 4) pregnancy
N total at baseline: Intervention 1: 145 Intervention 2: 154 Control 1: 142 Control 2: 151
Important prognostic factors2: For example age ± SD: I1: 64 ± 13 I2: 65 ± 13 C1: 65 ± 13 C2: 65 ± 12
Sex: I1: 72% M I2: 75% M C1: 75% M C2: 77% M
eGFR ml/min I1: 80 ± 26 I2: 82 ± 24 C1: 81 ± 23 C2: 82 ± 25
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
I1: sodium bicarbonate solution 1 ml/kg of body weight per hour for 12 h
I2: 3 ml/kg of body weight per hour for 1 h, followed by 1 ml/kg of body weight per hour for 11 h |
Describe control (treatment/procedure/test):
C1: Intravenous normal saline (0.9%) at a rate of 1 ml/kg of body weight per hour for 12 h
C2: normal saline at a rate of 3 ml/kg of body weight per hour for 1 h followed by 1 ml/kg of body weight per hour for 11 h |
Length of follow-up: 3 days – laboratory parameters 12 months – clinical events
Loss-to-follow-up: Not reported
Incomplete outcome data: Not reported
|
Outcome measures and effect size (include 95%CI and p-value if available):
sCr increase ≥25% compared to baseline I1: 24 (16%) I2: 27 (18%) C1: 29 (19%) C2: 27 (19%) P=0.92
sCr increase ≥0.5 mg/dL from baseline I1: 5 (3%) I2: 3 (3%) C1: 7 (5%) C2: 8 (6%) P=0.51
Mortality did not differ at 30 days and at 12 months (data not shown). |
Authors’ conclusion
In patients with STEMI undergoing PPCI, highvolume hydration with normal saline or sodium bicarbonate administrated at the time of contrast media administration was not associated with any significant advantage in terms of CI-AKI prevention. |
|
Ozcan, 2007 |
Type of study: randomized controlled trial
Setting: elective patients
Country: Turkey
Source of funding: not reported |
Inclusion criteria: patients who were scheduled for coronary angiography or percutaneous coronary intervention and had a baseline creatinine level N1.2 mg/dL
Exclusion criteria: 1) uncontrolled hypertension (systolic and diastolic blood pressure N160 mm Hg and N110 mm Hg, respectively), 2) emergency catheterization, 3) recent exposure to radiocontrast medium within 2 days, 4) volume overload, 5) serum creatinine levels >4 mg/dL
N total at baseline: Intervention: 88 Control: 88
Important prognostic factors2: For example age median (minimum – maximum) I: 68 (43-86) C: 70 (40-84)
Sex: I: 73% M C: 75% M
Creatinine clearance (mL/min) I: 53 (21 – 81) C: 50 (22-101)
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
1.4% sodium bicarbonate Iv fluid (1 mL/kg/h, upper limit 100 mL/h) for 6 hours before and 6 hours after the procedure
|
Describe control (treatment/procedure/test):
0.9% saline Iv fluid (1 mL/kg/h, upper limit 100 mL/h) for 6 hours before and 6 hours after the procedure
|
Length of follow-up: 48 hours
Loss-to-follow-up: Not reported
Incomplete outcome data: Not reported
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN (=an increase in serum creatinine N25% or 0.5 mg/dL after 48 hours) I: 12/88 C: 4/88 P=0.043 RR (adjusted): 0.29 95% CI: 0.09 – 0.96 |
Authors’ conclusion
Hydration with sodium bicarbonate provides better protection against CIN than the sodium chloride infusion does alone. |
|
Ratcliffe, 2009 |
Type of study: randomized controlled trial
Setting: elective patients, 1 center
Country: United States of America
Source of funding: not reported |
Inclusion criteria: 1) ambulatory or hospitalized patients who were scheduled for invasive coronary angiography or percutaneous coronary intervention for the evaluation and treatment of coronary artery disease 2) willing to participate in the study, and were able to understand and provide informed written consent 3) patients older than 18 years of age, with renal insufficiency defined by elevated serum creatinine (greater than 132.6 μmol/L in men, and greater than 114.9 μmol/L in women) or reduced calculated creatinine clearance (less than 1.002 mL/s) using the Cockcroft-Gault formula, and/or diabetes mellitus on oral antiglycemic or insulin therapy
Exclusion criteria: 1) pregnancy or lactation; 2) acute myocardial infarction; 3) clinical signs of heart failure (or documented ejection fraction of less than 35%); 4) cardiogenic shock; 5) hypertrophic or restrictive cardiomyopathy; 6) contrast medium exposure within one week before the procedure; 7) previous serious reactions to contrast medium; 8) renal transplantation; dialysis; severe comorbid illness; 9) use of dopamine, mannitol or fenoldopam; 10) newly discovered uncontrolled diabetes mellitus; 11) the inability to obtain informed consent or follow-up
N total at baseline: Intervention: Control:
Important prognostic factors2: For example age ± SD: I: 67 ± 11 C: 64 ± 10
Sex: I: 58% M C: 60% M
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
Iv 0.9% NaHCO3 hydration at an infusion rate of 3 mL/kg/h for 1 h before contrast, and continued at 1 mL/kg/h during the procedure and for 6 h following contrast exposure
|
Describe control (treatment/procedure/test):
Iv 0.9% saline hydration at an infusion rate of 3 mL/kg/h for 1 h before contrast, and continued at 1 mL/kg/h during the procedure and for 6 h following contrast exposure |
Length of follow-up: 72 hours
Loss-to-follow-up: Intervention: 15/30 (50%) Reasons: 11 lack of complete follow-up 4 other reasons
Control: 10/29 (30%) 8 lack of complete follow-up 2 other reasons
Incomplete outcome data: As above
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN (=an increase of greater than 25% in serum creatinine concentration from baseline to 72 h after administration of the contrast media) I: 2/19 (11%) C: 1/15 (7%) p>0.05
|
Authors’ conclusion:
CIN in high-risk patients may be effectively minimized solely through the use of an aggressive hydration protocol and an iso-osmolar contrast agent. The addition of NaHCO3 and/or NAC did not have an effect on the incidence of CIN. |
|
Recio-Mayoral, 2007 |
Type of study: randomized controlled trial
Setting: emergency patients, one hospital
Country: United Kingdom
Source of funding: not reported |
Inclusion criteria: 1) acute coronary syndrome (ACS) patients who were admitted to our coronary care unit 2) patients with myocardial infarction treated with primary PCI or rescue PCI, as well as patients with high-risk non–ST-segment elevation ACS needing urgent revascularization
Exclusion criteria: 1) end-stage renal failure on dialysis, 2) uncontrolled hypertension (systolic blood pressure >160 mm Hg and/or diastolic blood pressure >100 mm Hg) 3) signs of cardiac failure not responding to medical treatment, 4) known severe aortic valve stenosis (area >1.0 cm2), 5) allergy to iodated contrast or NAC 6) pregnancy
N total at baseline: Intervention: 56 Control: 55
Important prognostic factors2: For example age ± SD: I: 65 ± 10 C: 64 ± 9
Sex: I: 68% M C: 71% M
Glomerular filtration rate (mL/min) I: 75 ± 21 C: 74 ± 20
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
Active prophylactic treatment of PCI: Intravenous bolus of 5 ml/kg/h of alkaline saline solution with 154 mEq/l of sodium bicarbonate in 5% glucose and H2O (adding 77 ml of 1,000 mEq/l sodium bicarbonate to 433 ml of 5% glucose in H2O) plus 2,400 mg of N-AC in the same solution over 1 hour the bolus was administered in the 60 min preceding contrast injection Afterward, patients received fluid therapy, without N-AC, at 1.5 ml/kg/h perfusion rate in the 12 h after the procedure plus 2 doses of 600 mg N-AC orally the next day
|
Describe control (treatment/procedure/test):
Standard treatment: perfusion of isotonic saline (0.9%) at rate of 1 ml/kg/h for 12 h after PCI plus 2 doses of 600 mg N-AC orally the next day |
Length of follow-up: 3 days
Loss-to-follow-up: Not reported
Incomplete outcome data: Not reported
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN (=an absolute increase in SCr concentration of 0.5 mg/dl or more from baseline value in the 3 days after PCI) I: 1/55 (2%) C: 12/55 (22%) Odds ratio: 0.065 (95% CI: 0.008 – 0.521, p=0.01)
Acute anuric renal failure I: 1/55 (2%) C: 7/55 (13%) P=0.032 |
Authors’ conclusion:
Rapid intravenous hydration with sodium bicarbonate plus N-AC before contrast injection is effective and safe in the prevention of CIN in patients undergoing emergency PCI. |
|
Sodium bicarbonate short schedule versus saline long schedule for coronary angiography and/or percutaneous intervention |
|||||||
|
Briguori, 2007 |
Type of study: randomized controlled trial
Setting: elective patients, one hospital
Country: Italy
Source of funding: not reported |
Inclusion criteria: 1) patients with chronic kidney disease who underwent coronary and/or peripheral angiography and/or angioplasty 2) _18 years of age 3) stable serum creatinine concentration >2.0 mg/dL and/or or an estimated glomerular filtration rate <40 mL/ min/1.73 m2
Exclusion criteria: 1) serum creatinine levels >8 mg/dL, 2) a history of dialysis, 3) multiple myeloma, 4) pulmonary edema, 4) acute myocardial infarction, 5) recent exposure to radiographic contrast within 2 days of the study, 6) pregnancy, 7) administration of theophylline, dopamine, mannitol, or fenoldopam
N total at baseline: Intervention: 111 Control: 108
Important prognostic factors2: For example age ± SD: I: 70 ± 9 C: 71 ± 9
Sex: I: 88% M C: 81% M
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
154 mEq/L sodium bicarbonate in dextrose and H2O,. The initial intravenous bolus was 3 mL/kg/h for 1 hour immediately before contrast injection. After this, patients received the same fluid at a rate of 1 mL/kg/h during contrast exposure and for 6 hours after the procedure.
NAC orally at a dose of 1200 mg twice daily on the day before and the day of administration of the contrast agent (total of 2 days).
|
Describe control (treatment/procedure/test):
Isotonic saline (0.90%) was given intravenously at a rate of 1 mL/kg body weight per hour (0.5 mL/kg for patients with left ventricular ejection fraction _40%) for 12 hours before and 12 hours after administration of the contrast agent.
NAC orally at a dose of 1200 mg twice daily on the day before and the day of administration of the contrast agent (total of 2 days). |
Length of follow-up: 48 hours for laboratory parameters 5 days for clnical events
Loss-to-follow-up: Intervention: 9/117 (8%) 8 had no follow-up sCr value 1 had no contrast exposure
Control: 7/118(6%) 7 had no follow-up sCr value
Incomplete outcome data: As above
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN (=increase _25% of creatinine concentration) I: 2/108 (2%) C: 11/111 (10%) P=0.02
Renal failure requiring temporary dialysis: I: 1/108 (1%) C: 1/111 (1%) p-value not reported |
Authors’ conclusion:
The strategy of volume supplementation by sodium bicarbonate plus NAC seems to be superior to the combination of normal saline with NAC alone or with the addition of ascorbic acid in preventing CIN in patients at medium to high risk. |
|
Castini, 2008 |
Type of study: randomized controlled trial
Setting: one hospital
Country: Italy
Source of funding: not reported |
Inclusion criteria: 1) patients undergoing coronary angiography and/or percutaneous coronary intervention 2) aged 18 years or older with stable serum creatinine levels ≥1.2 mg/dL
Exclusion criteria: 1) serum creatinine levels >4 mg/dL, 2) a history of dialysis, 3) multiple myeloma, 4) pulmonary edema, 5) cardiogenic shock, 6) acute myocardial infarction, 7) emergency catheterization, 8) recent exposure to radiographic contrast media within 7 days of the study, 9) allergy to iodinate contrast media or NAC, 10) previous enrollment in the same or other protocols, 11) pregnancy, 12) administration of theophylline, mannitol, dopamine, dobutamine, nonsteroidal anti-inflammatory drugs, or fenoldopam.
N total at baseline: Intervention: 52 Control: 51
Important prognostic factors2: For example age ± SD: I: 70 ± 8 C: 73 ± 8
Sex: I: 85% M C: 84% M
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
154 mL of 1000 mEq/L SB added to 846 mL of 5% dextrose in H2O. The initial intravenous bolus was 3 mL/kg for 1 hour immediately before contrast injection. Thereafter, patients received the same fluid at a rate of 1 mL/kg per hour during contrast exposure and for 6 hours after the procedure.
|
Describe control (treatment/procedure/test):
saline (0.9%) given intravenously at a rate of 1 mL/kg body weight per hour for 12 hours before and 12 hours after administration of the contrast agent |
Length of follow-up: 5 days
Loss-to-follow-up: Not reported
Incomplete outcome data: Not reported
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN1 (=an increase in serum creatinine concentration≥25% over the baseline value in any of the 3 predefined time-points: 24 hours, 48 hours and 5 days) I: 7 (14%) C: 7 (14%) P>0.05
CIN2 (=the rate of an absolute increase in serum creatinine concentration ≥0.5 mg/dL at the same time-points) I: 6 (12%) C: 4 (8%) p>0.05
No patients required dialysis. |
Authors’ conclusion:
Our findings suggest that neither the addition of NAC nor the administration of SB add further benefit in CIN prevention, compared to standard hydration with isotonic saline infusion. |
|
Hafiz, 2012 |
Type of study: randomized controlled trial
Setting: elective patients, two tertiary hospitals
Country: United states of america
Source of funding: not reported |
Inclusion criteria: 1) patients undergoing elective coronary and peripheral angiography and intervention. 2) serum creatinine >1.6 mg/dl in non-diabetics and >1.4 mg/dl in diabetics or an estimated glomerular filtration rate (eGFR) of <50 ml/min/1.73 m2, calculated by the Modification of Diet in Renal Disease (MDRD) formula 3) age >18 years
Exclusion criteria: (1) were on dialysis; (2) had unstable renal function (defined as change in serum creatinine of >0.4 mg/dl within 48 hr prior to the index procedure), (3) had pulmonary edema, (4) had serum bicarbonate level >34 mmol/L; (5) received fenoldapam, mannitol, dopamine, or NAC within 48 hr prior to the index procedure; (6) were in cardiogenic shock, (7) were allergic to contrast media, (8) were pregnant, (9) were unable to provide informed consent.
N total at baseline: Intervention: 159 Control: 161
Important prognostic factors2: For example age (IQR): I: 74 (65-80) C: 73 (63-80)
Sex: I: 56% M C: 57% M
eGFR C: 41 (33-50)
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
dextrose 5% in water containing 154 mEq/L of NaHCO3 with or without NAC
NAC was used in 50% of patients in both study arms in a similarly randomized fashion as above; 1,200 mg was administered orally 2–12 hr before the procedure followed by another 1,200 mg oral dose 6–12 hr after the procedure |
Describe control (treatment/procedure/test):
intravenous 0.9% normal saline with or without NAC
NAC was used in 50% of patients in both study arms in a similarly randomized fashion as above; 1,200 mg was administered orally 2–12 hr before the procedure followed by another 1,200 mg oral dose 6–12 hr after the procedure |
Length of follow-up: 48 hours
Loss-to-follow-up: Not reported
Incomplete outcome data: Not reported
|
Outcome measures and effect size (include 95%CI and p-value if available):
CI-AKI (=increase in serum creatinine concentration of either >25% or >0.5 mg/dl at 48 hr after the procedure) I: 12% C: 9% p>0.05
There were no deaths or major adverse effects noted in our patient population during the study period. |
Authors’ coclusion:
Incidence of CI-AKI was no different in the NaHCO3 group compared to saline group, and NAC did not reduce CI-AKI in the two study arms. |
|
Klima, 2012 |
Type of study: randomized controlled trial
Setting: elective patients, multi-center trial
Country: Switzerland
Source of funding: commercial and non-commerzial |
Inclusion criteria: All patients admitted with renal dysfunction {actual serum creatinine level above the upper limit of normal of the serum creatinine (0.93 mmol/L for women and .117 mmol/L for men) or estimated glomerular filtration rate (eGFR) ,60 mL/min/1.73 m2 [eGFR calculated using the abbreviated Modification of Diet in Renal Disease (MDRD) study equation16]} scheduled to undergo an intra-arterial or intravenous radiographic contrast procedure on the next day
Exclusion criteria: 1) age ≥18 years, 2) pre-existing dialysis, allergy to radiographic contrast, 3) pregnancy, 4) severe heart failure (NYHA functional class III and IV), 5) N-acetylcysteine ≤24 h before contrast, 6) clinical condition requiring continuous fluid therapy, e.g. severe sepsis
N total at baseline: Intervention: 87 Control: 89
Important prognostic factors2: For example age median (IQR): I: 78 (70-82) C: 75 (70-82)
Sex: I: 66% M C: 62% M
eGFR ± SD I: 43 ± 11 C: 43 ± 12
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
The initial intravenous bolus was 3 mL/kg/h of 166 mEq/L sodium bicarbonate for 1 h immediately before radiocontrast injection. Following this, patients received the same fluid at a rate of 1 mL/kg/h during the contrast exposure and for 6 h after the procedure.
|
Describe control (treatment/procedure/test):
The infusion of 0.9% sodium chloride was administered at a continuous rate of 1 mL/kg/h, beginning from 8 p.m. on the day before the procedure and for at least 12h after the procedure. |
Length of follow-up: 48 hours
Loss-to-follow-up: Intervention: 6/93 (6%) 5 received no radiocontrast 1 refused participation
Control: 4/93 (4%) 4 received no radiocontrast
Incomplete outcome data: As above
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN (=an increase of ≥25% or an increase of ≥44 µmol/L in the baseline serum creatinine concentration within 48 h) I: 9% C:1% P=0.02
No patient experienced a serious adverse event related to the infusion (death, intensive care unit admission). Also, no patient required intravenous diuretics or nitrates due to pulmonary congestion. |
Authors’ conclusion:
Volume supplementation with 24 h sodium chloride 0.9% is superior to sodium bicarbonate for the prevention of CIN. |
|
Lee, 2011 |
Type of study: randomized controlled trial
Setting: elective patients, multicentre trial academic hospitals
Country: Korea
Source of funding: not reported |
Inclusion criteria: 1) patients undergoing coronary or endovascular angiography or intervention 2) serum creatinine ≥1.1 mg/dl, estimated glomerular filtration rate (eGFR) ≤60 ml/min/1.73 m2, 3) age ≥18 years, 4) diagnosis with diabetes mellitus
Exclusion criteria: 1) inability to obtain informed consent, 2) serum creatinine ≥8 mg/dl, eGFR ≤15 ml/min/1.73 m2 at rest, end-stage renal disease on hemodialysis, 3) multiple myeloma, 4) pulmonary edema, 5) uncontrolled hypertension (systolic pressure >160 mm Hg or diastolic pressure >100 mm Hg), 6) acute ST-segment elevation myocardial infarction while undergoing primary percutaneous intervention, 7) emergency coronary angioplasty or angiography, 8) use of contrast media within the previous 2 days, 9) pregnancy, 10) allergy to contrast medium 11) medications such as theophylline, dopamine, mannitol, fenoldopam, and NAC
N total at baseline: Intervention: 193 Control: 189
Important prognostic factors2: For example age median (IQR) I: 69 (63-73) C: 68 (67-72)
Sex: I: 70% M C: 71% M
eGFR: C: 46 (37-53)
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
Sodium bicarbonate infusion (154 mEq/L in dextrose and water) was begun 1 hour before the start of contrast injection, starting at 3 ml/kg/hour and decreasing to 1 ml/ kg/hour during the procedure and for 6 hours after completion of the procedure
All patients received NAC 1,200 mg 2 times/day for 2 days starting the day before the index procedure
|
Describe control (treatment/procedure/test):
0.9% sodium chloride 1 ml/kg/hour for 12 hours before and after the procedure
All patients received NAC 1,200 mg 2 times/day for 2 days starting the day before the index procedure
|
Length of follow-up: 48 hours for laboratory parameters 6 months for clinical parameters
Loss-to-follow-up: Intervention: 5/193 (3%) All had no laboratory data
Control: 2/189 (1%) All had no laboratory data
Incomplete outcome data: As above
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN (=a ≥25% increase in serum creatinine concentration or a ≥0.5 mg/dl absolute increase in serum creatinine from baseline within 48 hours after contrast exposure) I: 17 (9%) C: 10 (5%) P=0.17
Requirement of hemodialysis I: 4 (2%) C: 2 (1%) P=0.69
Rates of death, myocardial infarction, and stroke did not differ significantly at 1 month and 6 months after contrast exposure. |
Authors’ conclusion:
In conclusion, hydration with sodium bicarbonate is not superior to hydration with sodium chloride in preventing CIN in patients with diabetic nephropathy undergoing coronary or endovascular angiography or intervention.
Infusion rates were decreased to 0.5 ml/kg/hour in patients with left ventricular ejection fraction ≤45% in the 2 treatment arms. |
|
Maioli, 2008 |
Type of study: randomized controlled trial
Setting: elective patients, one center
Country: Italy
Source of funding: not reported |
Inclusion criteria: 1) patients with pre-angiographic estimated creatinin clearance <60 ml/min 2) undergoing planned angiographic procedures
Exclusion criteria: 1) creatinine clearance ≥ 60 ml/min n = 691 2) refusal to participate n = 18 3) administration of contrast medium within the previous 10 days n = 12 4) end stage renal disease n = 3
N total at baseline: Intervention: 250 Control: 252
Important prognostic factors2: For example age median (IQR): I: 74 (67-79) C: 74 (70-79)
Sex: I: 57% M C: 61% M
eGFR ± SD: I: 43 ± 11 C: 42 ± 10
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
Sodium bicarbonate (154 mEq/l in dextrose and water) received 3 ml/kg for 1 h before contrast medium, followed by an infusion of 1 ml/kg/h for 6 h after the procedure.
All patients received 600 mg oral NAC twice a day from the day before to the day after the procedure
|
Describe control (treatment/procedure/test):
1 ml/kg/h 0.9% sodium chloride for 12 h before and after the procedure |
Length of follow-up: 5 days
Loss-to-follow-up: Intervention: 4/252 (2%) 3 died 1 acute renal failure
Control: 5/250 (2%) 4 died 1 acute renal failure
Incomplete outcome data: As above
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN (=an absolute increase of at least 0.5 mg/dl over baseline serum creatinine within 5 days after the administration of the contrast medium) I: 25 (10%) C: 29 (12%) P=0.60
CIN2 (=as a relative increase _25% over baseline serum creatinine within 5 days after contrast agent administration) I: 15% C: 21% P=0.13
Death and acute renal failure, see column “Follow-up” for numbers, no significant difference in clinical events.
|
Authors’ conclusion:
Hydration with sodium bicarbonate plus NAC before contrast medium exposure is not more effective than hydration with isotonic saline plus NAC for prophylaxis of CIN in patients with moderate-to-severe renal dysfunction. |
|
Nieto-Rios, 2014 |
Type of study: randomized controlled trial
Setting: elective patients, single center
Country: Colombia
Source of funding: not reported |
Inclusion criteria: 1) Inpatients in a tertiary center, scheduled to undergo a procedure with the nonionic radiographic contrast agent iohexol. 2) serum creatinine levels of at least 1.2 mg/dL (106.1 μmol/L) and/or type 2 diabetics,
Exclusion criteria: 1) current clinical diagnosis of exacerbated congestive heart failure, 2) ejection fraction <35% by previous echocardiography, 3) signs of acute pulmonary edema within 48 hours before the procedure, 4) systolic blood pressure <90 mmHg or requirement of vasopressors support, 5) patients with exposure to contrast 30 days prior to the study, 6) known allergy to contrast dye, 7) chronic renal disease with dialysis therapy, 8) criteria for dialytic urgency, 9) pregnancy, 10) requirement of an emergency procedure (e.g., aortography for diagnosis of aortic aneurism), 11) patients with serum potassium <3 mEq/L (because of the risk of hypokalemia induced by bicarbonate), 12) uncompensated diabetes mellitus (four different values >200 mg/dL in the previous 24 hours) 13) patient or physician refusal to participate.
N total at baseline: Intervention: 107 Control: 113
Important prognostic factors2: For example age ± SD: I: 61 ± 17 C: 60 ± 17
Sex: I: 57% M C: 58% M
Baseline sCr (mg/dL): I: 1.3 ± 0.3 C: 1.3 ± 0.3
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
3 ml/kg of sodium bicarbonate solution (150 mEq/L) one hour prior to procedure and then drip rate was decreased to 1 ml/ kg/hour until 6 hours post procedure
|
Describe control (treatment/procedure/test):
1 ml/ kg/hour of normal saline solution, starting 12 hours before and continuing 12 hours after iohexol contrast |
Length of follow-up: 5 days
Loss-to-follow-up: Intervention: 7/107 (7%) 3 died 1 withdrawed 3 technical difficulties
Control: 1/113 (1%) 1 died
Incomplete outcome data: As above
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN (= increase in serum creatinine on 25% or more within 2 days after administration of radiographic contrast) I: 12 (12%) C: 8 (7%) RR: 1.68, 95% CI: 0.72 – 3.94 p>0.05
Decompensated heart failure I: 3 (3%) C: 7 (6%) P=0.34
|
Authors conclusion:
Our investigation showed that there were no differences between normal saline solution (extended infusion) vs. bicarbonate solution for nephroprotection. |
|
Shavit, 2009 |
Type of study: randomized controlled trial
Setting: elective patiens, single-center
Country: Israel
Source of funding: not reported |
Inclusion criteria: 1) patients with chronic kidney disease (CKD) stage III–IV undergoing cardiac catheterization
Exclusion criteria: 1) plasma creatinine levels more than 8 mg/dL or eGFR less than 15 mL/min, change in plasma creatinine levels of ≥0.5 mg/dL during the previous 24 hours, 2) preexisting dialysis, multiple myeloma, 3) pulmonary edema, 4) uncontrolled hypertension (systolic >160 mmHg, diastolic >100 mmHg), 5) recent exposure to radiographic contrast, or other nephrotoxic medications (within 2 days of the study), 6) allergy to radiocontrast, 7) pregnancy
N total at baseline: Intervention: 51 Control: 36
Important prognostic factors2: For example age ± SD: I: 72 ± 10 C: 71 ± 9
Sex: I: 84% M C: 70% M
eGFR (ml/min/1.73m2) ± SD: I: 43 ± 11 C: 40 ± 10
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
154 mEq/L sodium bicarbonate in 5% dextrose in water mixed by adding 154 mL of 1,000 mEq/L sodium bicarbonate to 846 mL of 5% dextrose in water. The initial IV bolus was 3 mL/kg for 1 hour before cardiac catheterization. Following this bolus, patients received the same fluid at a rate of 1 mL/kg per hour during the contrast exposure and for 6 hours after the procedure.
For patients weighing more than 110 kg, the initial fluid bolus and drip were limited to those doses administered to patients weighing 110 kg.
|
Describe control (treatment/procedure/test):
12-hour infusion of 154 mEq/L (0.9%) sodium chloride at a rate of 1 mL/kg per hour before cardiac catheterization and NAC 600 mg × 2/d orally the day before and the day of the procedure |
Length of follow-up: 2 days
Loss-to-follow-up: Intervention: 0 (0%)
Control: 5/41 (12%) No laboratory evaluation at baseline or after contrast exposure
Incomplete outcome data: As above
|
Outcome measures and effect size (include 95%CI and p-value if available):
CI-AKI 2 days of contrast administration) I: 5/51 (10%) C: 3/36 (8%) p>0.05
CI-AKI2 (=an increase in plasma creatinine of 0.3 mg/dL or more from baseline) C: 16% P>0.05
No patient developed more than 50% increment of creatinine or required renal replacement therapy during the hospitalization. |
Authors’ conclusion:
Hydration with sodium bicarbonate is not more effective than hydration with sodium chloride and oral NAC for prophylaxis of CI-AKI in patients with CKD stage III–IV undergoing cardiac catheterization. |
|
Sodium bicarbonate versus saline: “other schedules” for coronary angiography and/or percutaneous intervention |
|||||||
|
Chong, 2015 |
Type of study: randomized controlled trial
Setting: University Heart Centre Country: Singapore
Source of funding: not reported |
Inclusion criteria: 1) adults >21 years of age; 2) glomerular filtration rate (GFR) of 15–60 mL/min/1.73m2 – calculated by the abbreviated Modification of Diet in Renal Disease (MDRD) formula – 3) scheduled to undergo elective cardiac catheterisation with or without PCI 4) were able to receive pre-hydration for 12 h.
Exclusion criteria: 1) end-stage renal failure with GFR of b15 mL/min/1.73 m2, acute renal failure with a N44 μmol/L increase in serum Cr levels in the previous 24 h; 2) pre-existing dialysis; 3) pulmonary oedema or moderate to severe congestive heart failure (New York Heart Association III–IV); 4) inability to withstand the fluid load; 5) presence of haemodynamic compromise, uncontrolled hypertension (untreated systolic blood pressure N160mmHg, or diastolic blood pressure N100mmHg) 6) emergency cardiac catheterisation 7) exposure to contrast in the previous two days; 8) allergies to contrast or NAC; 9) administration of sodium bicarbonate or NAC within 48 h of cardiac catheterisation; 10) clinical conditions requiring continuous fluid therapy such as severe sepsis; 11) Use of potentially renal-toxic drugs; 12) cisplatin within 48 h of cardiac catheterisation and throughout the study duration;
Important prognostic factors2: For example age ± SD: I: 69 ± 10 I2: 71 ± 10 C: 67 ± 10
Sex: I1: 72% M I2: 78% M C: 78% M
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
I1: High-dose oral NAC with a sustained intravenous sodium chloride infusion (NAC group)
I2: Intravenous sodium bicarbonate infusion (SOB group) |
Describe control (treatment/procedure/test):
C1: Oral NAC and abbreviated intravenous sodium bicarbonate infusion (COM group) |
Length of follow-up: 48 hrs
Loss-to-follow-up: I1: 28/185 I2: 29/182 C1: 25/181
Death: I1: 0/185 I2: 1/182 C1: 2/181
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN, which was defined as ≥25% increase of serum Cr concentration or a ≥44 μmol/L (0.5mg/dL) increase in serum Cr within 48 h of cardiac catheterisation or PCI
I1: 6.5% I2: 12.8% C1: 10.6% P=0.214
|
Authors’ conclusion
‘The combination regimenwas not superior to individual regimens in preventing CIN in patientswith baseline renal impairment. There was a trend suggesting that the 12-hour sustained sodium chloride prehydration regimen was more protective than the 1-hour abbreviated SOB regimen.’ |
|
Motohiro, 2011 |
Type of study: randomized controlled trial
Setting: elective patient, 2 hospitals
Country: Japan
Source of funding: not reported |
Inclusion criteria: 1) patients undergoing coronary angiography or intervention 2) ≥20 years old 3) had an estimated glomerular filtration rate (eGFR) <60 ml/min/1.73 m2
Exclusion criteria: 1) serum creatinine levels >4 mg/dl, 2) changes in serum creatinine levels of ≥0.5 mg/dl during the previous 24 hours, 3) pre-existing dialysis, 4) pulmonary edema, 5) uncontrolled hypertension (treated systolic blood pressure >160 mm Hg or diastolic blood pressure >100 mm Hg), 6) emergency catheterization, 7) exposure to radiographic contrast within previous 2 days, 8) any allergy to radiographic contrast medium
N total at baseline: Intervention: 77 Control: 78
Important prognostic factors2: For example age ± SD: I: 74 ± 7 C: 71 ± 9
Sex: I: 64% M C: 76% M
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
0.9% sodium chloride for 12 hours before and after the procedure.
Sodium bicarbonate solution was prepared by adding 154 ml of sodium bicarbonate 1,000 mEq/L to 846 ml of 5% dextrose in water. In the sodium bicarbonate group the sodium bicarbonate solution was changed 3 hours before contrast administration
|
Describe control (treatment/procedure/test):
0.9% sodium chloride for 12 hours before and after the procedure. |
Length of follow-up: 1 months
Loss-to-follow-up: Intervention: 2/79 (2%) No laboratory test results
Control: 1/79 (1%) Angialgia due to sodium bicarbonate infusion
Incomplete outcome data: As above
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN (=25% increase or an absolute increase of _0.5 mg/dl in serum creatinine from baseline value, which appeared within 2 days of the produce) I: 2 (3%) P=0.02 relative risk 0.176, 95% confidence interval 0.037 to 0.83
No patient required Hemodialysis. |
Authors’ conclusion
Sodium chloride plus sodium bicarbonate is more effective than sodium chloride alone for prophylaxis of CIN and can lead to retention of better long-term renal function. |
|
Tamura, 2009 |
Type of study: randomized controlled trial
Setting: elective patients, two hospitals
Country: Japan
Source of funding: not reported |
Inclusion criteria: 1) Patients who were scheduled for elective coronary arteriography or percutaneous coronary intervention 2) age >20 years 3) serum creatinine (Cr) level >1.1 to <2.0 mg/dl.
Exclusion criteria: 1) allergy to contrast medium, pregnancy, 2) history of dialysis, 3) exposure to contrast-medium within the preceding 48 hours of the study, 4) acute coronary syndrome within the preceding 1 month of the study, 5) severe symptoms of heart failure (New York Heart Association functional class IV), 6) left ventricular ejection fraction >25%, 7) severe chronic respiratory disease, 8) single functioning kidney, 9) administration of N-acetylcysteine, theophylline, dopamine, or mannitol
N total at baseline: Intervention: 72 Control: 72
Important prognostic factors2: For example age ± SD: I: 73 ± 8 C: 72 ± 10
Sex: I: 83% M C: 92% M
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
Standard hydration with sodium chloride plus single-bolus intravenous administration of sodium bicarbonate (20 ml /20 mEq; Meyron 84, Otsuka Pharmaceutical, Inc., Tokyo, Japan) 5 minutes before contrast exposure
|
Describe control (treatment/procedure/test):
Standard hydration with sodium chloride alone
(=intravenous administration with isotonic saline (0.9%) at a rate of 1 ml/kg/hour (0.5 ml/kg/hour for patients with left ventricular ejection fraction <40%) for 12 hours before and 12 hours after an elective coronary procedure. For patients weighing >80 kg, infusion rate was limited to 80 ml/hour (40 ml/hour for patients with left ventricular ejection fraction _40%).
|
Length of follow-up: 3 days
Loss-to-follow-up: All patients completed the study
Incomplete outcome data: All patients completed the study
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN (=an increase ≥25% or ≥0.5 mg/dl in serum Cr within the first 3 days after the procedure compared to baseline value) I: 1.4% C: 12.5% P=0.017
Adverse clinical events (acute pulmonary edema, acute renal failure requiring dialysis, and death within 7 days of procedure) I: 0% C: 1.4% p>0.05 |
Authors’ conclusion
In conclusion, single-bolus intravenous administration of sodium bicarbonate in addition to standard hydration can more effectively prevent CIN than standard hydration alone in patients with mild renal insufficiency undergoing an elective coronary procedure. |
|
Turedi, 2016 |
Type of study: randomized controlled trial
Setting: academic emergency center
Country: Turkey
Source of funding: not reported |
Inclusion criteria: 1) Undergoing contrastenhanced thoracic CT due to suspected PE; 2) aged over 18 years; 3) with measure-able basal creatinine levels pretomography and; 4) measureable serum creatinine levels 48– 72 hours posttomography, and with one or more of the risk factors for CIN. The risk factors were preexisting renal dysfunction (Cr 1.4 mg/dL or a high or calculated glomerular filtration rate [GFR] < 60 mL/min/1.73 m2), diabetes mellitus, hypertension receiving treatment, hypotension (systolic blood pressure < 90 mm Hg), coronary artery disease, history of nephrotoxic drug use (nonsteroidal anti-inflammatory drugs, cisplatin, aminoglycoside, amphotericin B), liver disease, congestive heart failure (active or history thereof), age 75 or over, and anemia (hematocrit < 30%).
Exclusion criteria: 1) end-stage renal disease already in peritoneal dialysis; 2) hemodialysis; 3) pregnant women; 4) subjects with a known allergy to NAC or NaHCO3; 5) patients requiring NAC therapy or NaHCO3 therapy for existing additional disease; 6) exposed to contrast material for any reason in the previous 10 days or 7) during the in-hospital follow-up period 8) patients who refused to participate
Important prognostic factors2: For example age ± SD: I: 76 (72-80) I2: 77 (71-80) C: 74 (73-76)
Sex: I1: 48% M I2: 51% M C: 53% M
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
I1: 3 mL/kg intavenous NAC+NS solution (3 g NAC was made up to 1000 mL with NS),
I2: NaHCO3 + NS solution (132 mEq NaHCO3 was made up to 1000 mL with NS)
|
Describe control (treatment/procedure/test):
C1: NS alone 1 hour before CTPA and 1 mL/kg intavenous per hour for a minimum of 6 hour after CTPA. |
Length of follow-up: 48-72 hrs
Loss-to-follow-up: I1: 7/85 I2: 8/85 C1: 11/87
Death: I1: 4/85 I2: 2/85 C1: 6/87
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN development creatinine levels and post-CTPA creatinine levels measured 48–72 hours following contrast exposure and an increase ≥25% or 0.5 mg/dL
I1: 23.5% I2: 21.2% C1: 26.4% P=0.719
|
Authors’ conclusion
‘In conclusion, there were no statistically significant differences observed among prophylactic NAC, NaHCO3, and NS in prevention of CIN following contrast-enhanced CTPA.’ |
|
Ueda, 2011 |
Type of study: randomized controlled trial
Setting: emergency patients, single center
Country: Japan
Source of funding: not reported |
Inclusion criteria: 1) patients undergoing an emergent (within 60 minutes of admission) diagnostic or interventional coronary procedure, such as coronary angiography or percutaneous coronary intervention 2) >20 years old 3) had renal insufficiency, defined by a serum creatinine (Cr) concentration of >1.1 mg/dl or estimated glomerual filtration rate (eGFR) of <60 ml/min
Exclusion criteria: 1) change in the serum Cr concentration of >0.5 mg/dl during the 24 hours before the procedure, 2) pre-existing dialysis, exposure to the contrast media within 2 days before the study, 3) allergy to the contrast media, pregnancy, 4) previous or planned administration of mannitol, fenoldopam, N-acetylcysteine, theophylline, dopamine, or nonstudy sodium bicarbonate
N total at baseline: Intervention: 30 Control: 29
Important prognostic factors2: For example age ± SD: I: 77 ± 9 C: 75 ± 10
Sex: I: 79% M C: 77% M
sCr (mg/dL) ± SD: I: 1.32 ± 0.46 C: 1.51 ± 0.59
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
Intravenous bolus injection of 154 mEq/L of sodium bicarbonate at a dose of 0.5 ml/kg, as soon as possible after they were admitted, before the administration of the contrast medium
Intravenous infusion of 154 mEq/L sodium bicarbonate at 1 ml/kg/hour during and for 6 hours after the coronary procedure
|
Describe control (treatment/procedure/test):
Intravenous bolus injection of 154 mEq/L of sodium chloride at a dose of 0.5 ml/kg, as soon as possible after they were admitted, before the administration of the contrast medium
Intravenous infusion of 154 mEq/L sodium bicarbonate at 1 ml/kg/hour during and for 6 hours after the coronary procedure
|
Length of follow-up: 2 days
Loss-to-follow-up: Intervention: 0 (0%)
Control: 1/30 (3%) Circulatory failure
Incomplete outcome data: As above
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN (=an increase by >25% or >0.5 mg/dl of the serum creatinine level within 2 days after the procedure) I: 1 (3%) C: 8 (28%) RR: 0.12, 95% CI: 0.016 – 0.91 P=0.01
Congestive heart failure I: 5/30 (17%) C: 6/29 (21%) p>0.05
Death I: 2/30 (7%) C: 2/29 (7%) p>0.05
No patients developed acute renal failure requiring hemodialysis. |
Authors’ conclusion
In conclusion, rapid alkalization by bolus injection of sodium bicarbonate was effective for the prevention of CIN in patients with CKD undergoing emergent procedures. |
|
Sodium bicarbonate short schedule versus saline long schedule for computed tomography |
|||||||
|
Kooiman, 2014 |
Type of study: randomized controlled trial
Setting: elective patients, multi-center trial
Country: the Netherlands
Source of funding: non-commercial |
Inclusion criteria: 1) In- and outpatients electively scheduled for CE-CT regardless of the indication 2) least 18 years of age, had CKD (eGFR <60 mL/min/1.73 m2 estimated by the Modification of Diet in Renal Disease formula 3) eligible for the fluid challenge of saline hydration
Exclusion criteria: 1) pregnancy, 2) previous contrast administration within the last 7 days, 3) documented allergy for iodinated contrast media, 4) haemodynamic instability (systolic blood pressure <100 mmHg) 5) previous participation in the trial
N total at baseline: Intervention: 267 Control: 281
Important prognostic factors2: For example age ± SD: I: 72 ± 10 C: 73 ± 10
Sex: I: 60% M C: 61% M
Mean eGFR: I: 50 ± 13 C: 51 ± 14
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
250 mL intravenous 1.4% sodium bicarbonate 1 h prior to CE-CT without hydration post-CE-CT
|
Describe control (treatment/procedure/test):
2000 mL of intravenous 0.9% saline, 1000 mL prior to and 1000 mL post-CE-CT |
Length of follow-up: 96 hours
Loss-to-follow-up: Intervention: 15/267(6%) 2 treated according to protocol 5 CT without iv contrast 6 CT cancelled and no hydration
Control: 20/281 (7%) 7 treated according to protocol 7 CT cancelled and no hydration 4 CT without iv contrast 2 treated with sodium bicarbonate
Incomplete outcome data: As above
|
Outcome measures and effect size (include 95%CI and p-value if available):
CI-AKI (=serum creatinine increase >25%/>44 μmol/L (0.5 mg/dL) I: 8 (3%) C: 14 (5%) P=0.23
Recovery of kidney function: I: 75% C: 69% P=0.81
Acute heart failure due to volume expansion (based on the treating physician’s clinical judgement) occurred in none of the patients in the sodium bicarbonate group versus 6 of 281 patients in the saline group (P = 0.03)
None of the CI-AKI patients developed a need for dialysis. |
Authors’ conclusion
Short hydration with sodium bicarbonate prior to CE-CT was non-inferior to peri-procedural saline hydration with respect to renal safety and may result in healthcare savings. |
|
Controlled diuresis for coronary angiography and/or percutaneous intervention |
|||||||
|
Barbanti, 2016 |
Type of study: randomized controlled trial
Setting: university hospital
Country: Italy
Source of funding: not reported |
Inclusion criteria: 1) All patients with symptomatic severe aortic stenosis undergoing TAVI were considered eligible Exclusion criteria: 1) chronic end-stage renal failure on dialysis; 2) episode of acute congestive heart failure with left ventricular ejection fraction <30% in the past 30 days before randomization; 3) contraindica-tions to placement of a Foley catheter; 4) urgent TAVI 5) unavailability of the RenalGuard system.
Important prognostic factors2: For example age ± SD: I: 82 (78-83) C: 81 (78-84)
Sex: I: 61% F C: 59% F
Serum creatine ± SD I: 1.0 (0.85-1.15) C: 0.97 (0.83-1.16)
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
RenalGuard therapy received hydration with a normal saline solution; with an initial bolus (priming) of 250 ml was infused over 30 min (preprocedural. Urine flow was monitored and maintained at the target value throughout the procedure and during the following 4 h. phase). |
Describe control (treatment/procedure/test):
control group received sodium normal saline solution at a rate of 1 ml/kg/h 12 h before TAVR, during contrast exposure, and for 6 h after the procedure. |
Length of follow-up: 78 hrs
Loss-to-follow-up: No loss to follow-up
|
Outcome measures and effect size (include 95%CI and p-value if available):
AKI (defined: absolute reduction in kidney function (<72 h) and defined as: 1) stage 1: increase in serum creatinine to 150% to 200% (1.5 to 2.0x increase compared with baseline) or increase of >0.3 mg/dl (≥26.4 mmol/l); 2) stage 2: increase in serum creatinine to 200% to 300% (2.0 to 3.0x increase compared with baseline); and 3) stage 3: increase in serum creatinine to ≥300% (>3_ increase compared with baseline) or serum creatinine of ≥4.0 mg/dl (≥354 mmol/l) with an acute increase of at least 0.5 mg/dl (44 mmol/l).)
I: 4 (5.4%) C: 13 (25.2%) RR: 0.21, 95% CI: 0.06 – 0.71 P=0.014
Cardiovascular death I: 0/56(0%) C: 1/56 (1.8%) P=0.306
Death I: 1/56 (1.8%) C: 2/56 (3.6%) P=0.537 |
Authors’ conclusion
‘In summary, furosemide-induced diuresis with matched isotonic intravenous hydration using the RenalGuard system is an effective therapeutic tool to reduce the occurrence of AKI in patients undergoing TAVR.’ |
|
Brar, 2014 |
Type of study: randomized controlled trial
Setting: elective patients, 1 center
Country: United states of America
Source of funding: not reported |
Inclusion criteria: 1) patients referred to the cardiac catheterisation laboratory 2) an estimated glomerular fi ltration rate (GFR) of 60 mL/min per 1・73 m2 or lower; 3) age 18 years or older; 4) at least one of the following: diabetes mellitus, history of congestive heart failure, hypertension (blood pressure >140/90 mm Hg or treatment with antihypertensive medication), or age older than 75 years.
Exclusion criteria: 1) inability to obtain consent from participants, 2) emergency cardiac catheterisation (eg, primary percutaneous coronary intervention for ST-segment elevation myocardial infarction), 3) renal replacement therapy, 4) exposure to radiographic contrast media within the previous 2 days, 5) allergy to radiographic contrast media, 6) acute decompensated heart failure, 7) severe valvular heart disease, 8) mechanical aortic prosthesis, 9) left ventricular thrombus, 10) history of kidney or heart transplantation, 11) change in estimated GFR of 7.5% or more per day or a cumulative change of 15% or more during the pre ceding 2 or more days.
N total at baseline: Intervention: 196 Control: 200
Important prognostic factors2: For example age ± SD: I: 71 ± 9 C: 72 ± 8
Sex: I: 64% M C: 59% M
eGFR ± SD I: 48 ± 9 C: 48 ± 9
Groups comparable at baseline? |
Describe intervention (treatment/procedure/test):
0.9% sodium chloride bolus infusion at 3 mL/kg for 1 h
The fl uid rate was adjusted according to the left ventricular end-diastolic pressure as follows: 5 mL/kg/h for left ventricular end-diastolic pressure lower than 13 mmHg, 3 mL/kg/h for pressure of 13–18 mmHg, and 1.5 mL/kg/h for pressure higher than 18 mmHg. The fl uid rate was set at the start of the procedure (before contrast exposure), continued for the duration of the procedure, and for 4 h post-procedure. |
Describe control (treatment/procedure/test):
0.9% sodium chloride bolus infusion at 3 mL/kg for 1 h
5 mL/kg per h. The fl uid rate was set at the start of the procedure (before contrast exposure), continued for the duration of the procedure, and for 4 h post-procedure. |
Length of follow-up: 2-8 weeks for laboratory parameters 6 months for clinical events
Loss-to-follow-up: Intervention: 0 (0%)
Control: 0 (0%)
Incomplete outcome data: Intervention: 18/196 (9%) 12 had 1 sCr value 6 had no sCr value
Control: 28/200 (14%) 24 had 1 sCr value 4 had no sCr value
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN (=a greater than 25% or 0.5 mg/dL increase in the serum creatinine concentration) I: 12/178 (7%) C: 28/172 (16%) RR: 0.41, 95% CI: 0.22 – 0.79, p=0.005
6-months mortality I: 0.5% C: 4% P=0.037
No significant difference in other adverse clinical events at 30 days or 6 months
In total, six patients (1・5%)—three in each group— terminated the intravenous fl uids early, the reason for which was shortness of breath in all six patients. |
Authors’ conclusion:
Left ventricular end-diastolic pressure-guided fl uid administration seems to be safe and eff ective in preventing contrast-induced acute kidney injury in patients undergoing cardiac catheterisation. |
|
Briguori, 2011 |
Type of study: randomized controlled trial
Setting: elective patients, multicenter
Country: Italy
Source of funding: not reported |
Inclusion criteria: 1) patients with chronic kidney disease scheduled for coronary and/or peripheral angiography and/or angioplasty with an estimated glomerular filtration rate (eGFR) ≤30mL /min/ 1.73 m2 and/or a risk score ≥11)
Exclusion criteria: 1) acute myocardial infarction; 2) acute pulmonary edema; 3) cardiogenic shock; 4) dialysis; 5) multiple myeloma; 6) administration of sodium bicarbonate, theophilline, dopamine, mannitol, and/or fenoldopam; 7) recent (<48 hours) administration of iodinated contrast medium 8) enrollement in another study
N total at baseline: Intervention: 146 Control: 146
Important prognostic factors2: For example age ± SD: I: 76 ± 8 C: 75 ± 9
Sex: I: 61% M C: 71% M
eGFR ± SD: I: 32 ± 7 C: 32 ± 9
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
hydration with normal saline plus NAC controlled by the RenalGuard system
NAC was administered only iv (1500 mg in 1L saline) during the 3 phases (preprocedural, intraprocedural, and postprocedural) of the RenalGuard therapy.
|
Describe control (treatment/procedure/test):
154 mEq/L sodium bicarbonate in dextrose and H2O. The initial intravenous bolus was 3 mL/kg per hour for at least 1 hour before contrast injection. Then, all patients received the same fluid at a rate of 1 mL/kg per hour during contrast exposure and for 6 hours after the procedure.
NAC orally at a dose of 1200 mg twice daily the day before and the day of administration of the contrast agent (for a total of 2 days) additional NAC dose (1200 mg diluted in 100 mL normal saline) was administered intravenously during the procedure. The total NAC dose was 6 g. |
Length of follow-up: 1 week
Loss-to-follow-up: 0 (0%) in both groups
Incomplete outcome data: Intervention: 0 (0%)
Control: 3/147 (2%) 2 discontinued treatment 1 did not receive allocated treatment
|
Outcome measures and effect size (include 95%CI and p-value if available):
CI-AKI (=an increase in sCr concentration ≥0.3 mg/dL above the baseline value at 48 hours after administration of Contrast or the need fordialysis) C: 30/146 (21%) Odds ratio: 0.47, 95% CI 0.24 – 0.92 P<0.05 |
Authors’ conclusion:
RenalGuard therapy is superior to sodium bicarbonate and N-acetylcysteine in preventing contrast-induced acute kidney injury in high-risk patients.
The risk score for predicting CI-AKI was calculated according to the following algorithm: hypotension (integer score 5), intra-aortic balloon pump support (integer score 5), congestive heart failure (integer score 4), age >75 years (integer score 4), diabetes mellitus (integer score 3), eGFR _60 mL/min/1.73 m2 (integer score 2 to 6), preexisting anemia(integer score 3), and CM volume (integer score 1 for each 100 cm3). The global scores ≥5, 6 to 10, 11 to 16, and _16 predict a CI-AKI risk of 7.5%, 14%, 26.1%, and 57.3%, respectively.
|
|
Marenzi, 2012 |
Type of study: randomised controlled trial
Setting: elective and emergency patients
Country: Italy
Source of funding: not reported |
Inclusion criteria: 1) age ≥18 years and ≤85 years, and elective or urgent (within 24 h from hospital admission because of non–ST-segment elevation [acute] myocardial infarction [NSTEMI]) coronary angiography and, when indicated, percutaneous coronary intervention (PCI).
Exclusion criteria: 1) primary or rescue PCI and angiography procedures requiring a direct renal injection of contrast, 2) cardiogenic shock, overt congestive heart failure, 3) acute respiratory insufficiency, 4) recent acute kidney injury, 5) chronic peritoneal or hemodialysis treatment, 6) known furosemide hypersensitivity, 7) receipt of intravenous contrast within 10 days before the procedure or another planned contrast-enhanced procedure in the following 72 h, 8) contraindications to placement of a Foley catheter in the bladder.
N total at baseline: Intervention: 87 Control: 83
Important prognostic factors2: For example age ± SD: I: 73 ± 7 C: 74 ± 8
Sex: I: 78% M C: 78% M
eGFR ± SD: C: 1.7 ± 0.5
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
Approximately 90 min before the coronary procedure, Furosemide with matched hydration treatment was started with an initial intravenous bolus (250 ml) of normal saline solution over 30 min. Furosemide was then administered as a single intravenous bolus of 0.5 mg/kg (up to a maximum of 50 mg). Urine output was calculated continuously by the system, and when a urine output rate >300 ml/h was achieved, patients were brought to the catheterization laboratory and underwent coronary angiography. Matched hydration was continued throughout the catheterization procedure and for 4 h after the last contrast dose. At this time, therapy was discontinued. Additional doses of furosemide (up to a maximal cumulative dose of 2.0 mg/kg) were given in cases where the urine output was below 300 ml/h during treatment. The Foley catheter was removed 24 h after the procedure.
|
Describe control (treatment/procedure/test):
continuous intravenous infusion of isotonic saline at a rate of 1 ml/kg/h (0.5ml/kg/h in case of left ventricular ejection fraction ≤40%) for at least 12 h before and 12 h after the procedure. |
Length of follow-up: 72 hours
Loss-to-follow-up: Intervention: 2/89 (2%) Failed to insert foley catheter
Control: 2/85 (2%) Withdrawal of treatment due to pulmonary edema
Incomplete outcome data: As described above)
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN (=a ≥25% or ≥0.5 mg/dl rise in serum creatinine over baseline during the first 72 h post-procedure) I: 4 (5%) C: 15 (18%) P=0.005
Cumulative in-hospital complications I: 8% C: 18% P=0.052 |
Authors’ conclusion:
In patients with CKD undergoing coronary procedures, furosemide-induced high urine output with matched hydration significantly reduces the risk of CIN and may be associated with improved in-hospital outcome. |
|
Qian, 2016 |
Type of study: randomised controlled trial
Setting: elective patients, multiple centers
Country: Japan
Source of funding: not reported |
Inclusion criteria: 1) patients with CKD and chronic heart failure undergoing coronary procedures
Exclusion criteria: -
N total at baseline: Intervention: 132 Control: 132
Groups comparable at baseline? Yes
|
Describe intervention (treatment/procedure/test):
Central-venous pressure guided hydration group
|
Describe control (treatment/procedure/test):
Standard hydration group |
Length of follow-up: 48 hours
Loss-to-follow-up: Not reported
Incomplete outcome data: Not reported
|
Outcome measures and effect size (include 95%CI and p-value if available):
CIN (=an increase by >25% or >0.5 mg/dl of the serum creatinine level within 2 days after the procedure) I: 16% C: 30% P=0.006
Acute heart failure: I: 3.8% C: 3.0% P=0.50 |
Authors’ conclusion:
Controlled vnous pressure guided fluid administration can safely and effectively reduce the risk of CIN in patients with CKD and chronic heart failure. |
|
Usmiani, 2015 |
Type of study: randomized controlled trial
Setting: elective patients
Country: Brazil
Source of funding: not reported |
Inclusion criteria: 1) patients with chronic kidney disease (CKD) undergoing coronary procedures
Exclusion criteria: -
N total at baseline: Intervention: 65 Control: 68
Groups comparable at baseline? Yes
|
Describe intervention (treatment/procedure/test):
iv 250 mL isotonic saline bolus, followed by a 0.5 mg/kg furosemide i.v. bolus to forced diuresis. A dedicated device automatically matched the isotonic saline i.v. infusion rate to the urinary output for 1 h before, during and 4 h after the procedure.
|
Describe control (treatment/procedure/test):
Standard saline and bicarbonate hydration |
Length of follow-up: 2 days
Loss-to-follow-up: Not reported
Incomplete outcome data: Not reported
|
Outcome measures and effect size (include 95%CI and p-value if available):
CI-AKI (=an increase by >25% or >0.5 mg/dl of the serum creatinine level within 2 days after the procedure) I: 7% C: 25% P=0.01
Major adverse cardiovascular events I: 7% C: 32% P<0.01 |
Authors’ conclusion:
In patients with CKD undergoing coronary procedures, furosemide-induced high urine output with matched hydration significantly reduces the risk of CIN and may be associated with improved in-hospital outcome. |
|
Usmiani, 2016 |
Type of study: randomized controlled trial
Setting: university hospital
Country: Italy
Source of funding: not reported |
Inclusion criteria: 1) Elgibile for voth procedures 2) eGFR of less than 60 mL/ min/1.73m2
Exclusion criteria: 1) primary PCI (emergency procedure); 2) cardiogenic shock; 3) acute heart failure; 4) endstage renal disease on haemodialysis; 5) urinary tract infections within the last 3 months; 6) benign prostatic hyperplasia and; 7) previously known difficulties in urinary catheterization.
Important prognostic factors2: For example age ± SD: I1: 76 ± 9 C: 75 ± 8
Sex: I1: 22% F C: 29% F
Serum creatine ± SD I1: 1.54 ±0.43 C: 1.42 ±0.41
Groups comparable at baseline? Yes |
Describe intervention (treatment/procedure/test):
Matched hydration was to be performed with the Renal- Guard System.
250 mL i.v. isotonic saline bolus is given in 30 min, followed by 0.5 mg/kg i.v. furosemide to forced diuresis. Isotonic saline i.v. infusion proceeds automatically, rate-matched with diuresis |
Describe control (treatment/procedure/test):
BS-NAC intravenous hydration (isotonic saline/ N-acetylcysteine/vitamin C)
1000 mL isotonic saline i.v. administration 12 h before procedure (rate-adjusted according to LVEF 20–40mL/h if LVEF<30%, 80–120 mL/h if LVEF 30–50%, 200 mL/h if LVEF >50%).
Plus 3 mL/kg/h 1.4% SB solution i.v. infusion for 1 h before Plus: 5000mg p.o. Vitamin C Plus: 1200mg p.o. N-acetylcysteine |
Length of follow-up: 7 days
Loss-to-follow-up: 9 loss to follow-up I: 8/67 C: 1/66
|
Outcome measures and effect size (include 95%CI and p-value if available):
AKI (CIAKI after coronary angiography/PCI as defined by an increase of sCr +0.3 mg/dL in 48 h or +50% in 7 days)
I: 4 (6%) C: 16 (24%) P=0.01
Cardiovascular death I: 1/59(1.7%) C: 7/65 (10.8%)
|
Authors’ conclusion
‘Matched hydration was more effective than BS-NAC in CIAKI prevention.’ |
Notes:
- Prognostic balance between treatment groups is usually guaranteed in randomized studies, but non-randomized (observational) studies require matching of patients between treatment groups (case-control studies) or multivariate adjustment for prognostic factors (confounders) (cohort studies); the evidence table should contain sufficient details on these procedures
- Provide data per treatment group on the most important prognostic factors [(potential) confounders]
- For case-control studies, provide sufficient detail on the procedure used to match cases and controls
- For cohort studies, provide sufficient detail on the (multivariate) analyses used to adjust for (potential) confounders
CAG: Cardiac angiography; CI-AKI: contrast-induced acute kidney injury; CIN: contrast induced nephropathy; CKD: chronic kidney disease; CT: computed tomography; CTPA: computed tomography – pulmonary angiography; ia: intra-arterial; IQR: intra quartile range; iv: intra-venous; NAC: N-acetylcysteine; PCI: percutaneous coronary intervention; sCr: serum creatinine
Verantwoording
Autorisatiedatum en geldigheid
Laatst beoordeeld : 01-11-2017
Laatst geautoriseerd : 01-11-2017
Geplande herbeoordeling : 01-12-2023
Validity
The board of the Radiological Society of the Netherlands will determine at the latest in 2023 if this guideline (per module) is still valid and applicable. If necessary, a new working group will be formed to revise the guideline. The validity of a guideline can be shorter than 5 years, if new scientific or healthcare structure developments arise, that could be seen as a reason to commence revisions. The Radiological Society of the Netherlands is considered the keeper of this guideline and thus primarily responsible for the actuality of the guideline. The other scientific societies that have participated in the guideline development share the responsibility to inform the primarily responsible scientific society about relevant developments in their field.
Initiative
Radiological Society of the Netherlands
Authorization
The guideline is submitted for authorization to:
- Association of Surgeons of the Netherlands
- Dutch Association of Urology
- Dutch Federation of Nephrology
- Dutch Society Medical Imaging and Radiotherapy
- Dutch Society of Intensive Care
- Netherlands Association of Internal Medici
- Netherlands Society for Clinical Chemistry and Laboratory Medicine
- Netherlands Society of Cardiology
- Netherlands Society of Emergency Physicians
- Radiological Society of the Netherlands
Algemene gegevens
General Information
The guideline development was assisted by the Knowledge Institute of Medical Specialists (https://www.kennisinstituut.nl) and was financed by the Quality Funds for Medical Specialists (Kwaliteitsgelden Medisch Specialisten: SKMS).
Doel en doelgroep
Goal of the current guideline
The aim of the Part 1 of Safe Use of Iodine-containing Contrast Media guidelines is to critically review the present recent evidence with the above trend in mind, and try to formulate new practical guidelines for all hospital physicians to provide the safe use of contrast media in diagnostic and interventional studies. The ultimate goal of this guideline is to increase the quality of care, by providing efficient and expedient healthcare to the specific patient populations that may benefit from this healthcare and simultaneously guard patients from ineffective care. Furthermore, such a guideline should ideally be able to save money and reduce day-hospital waiting lists.
Users of this guideline
This guideline is intended for all hospital physicians that request or perform diagnostic or interventional radiologic or cardiologic studies for their patients in which CM are involved.
Samenstelling werkgroep
Working group members
A multidisciplinary working group was formed for the development of the guideline in 2014. The working group consisted of representatives from all relevant medical specialization fields that are involved with intravascular contrast administration.
All working group members have been officially delegated for participation in the working group by their scientific societies. The working group has developed a guideline in the period from October 2014 until July 2017.
The working group is responsible for the complete text of this guideline.
Working group
Cobbaert C., clinical chemist, Leiden University Medical Centre (member of advisory board from September 2015)
Danse P., interventional cardiologist, Rijnstate Hospital, Arnhem
Dekker H.M., radiologist, Radboud University Medical Centre, Nijmegen
Geenen R.W.F., radiologist, Noordwest Ziekenhuisgroep (NWZ), Alkmaar/Den Helder
Hoogeveen E.K., nephrologist, Jeroen Bosch Hospital, ‘s-Hertogenbosch
Kooiman J., research physician, Leiden University Medical Centre, Leiden
Oudemans - van Straaten H.M., internist-intensive care specialist, Free University Medical Centre, Amsterdam
Pels Rijcken T.H., interventional radiologist, Tergooi, Hilversum
Sijpkens Y.W.J., nephrologist, Haaglanden Medical Centre, The Hague
Vainas T., vascular surgeon, University Medical Centre Groningen (until September 2015)
van den Meiracker A.H., internist-vascular medicine, Erasmus Medical Centre, Rotterdam
van der Molen A.J., radiologist, Leiden University Medical Centre, Leiden (chairman)
Wikkeling O.R.M., vascular surgeon, Heelkunde Friesland Groep, location: Nij Smellinghe Hospital, Drachten (from September 2015)
Advisory board
Demir A.Y., clinical chemist, Meander Medical Center, Amersfoort, (member of working group until September 2015)
Hubbers R., patient representative, Dutch Kidney Patient Association
Mazel J., urologist, Spaarne Gasthuis, Haarlem
Moos S., resident in Radiology, HAGA Hospital, The Hague
Prantl K., Coordinator Quality & Research, Dutch Kidney Patient Association
van den Wijngaard J., resident in Clinical Chemistry, Leiden University Medical Center
Methodological support
Boschman J., advisor, Knowledge Institute of Medical Specialists (from May 2017)
Burger K., senior advisor, Knowledge Institute of Medical Specialists (until March 2015)
Harmsen W., advisor, Knowledge Institute of Medical Specialists (from May 2017)
Mostovaya I.M., advisor, Knowledge Institute of Medical Specialists
Persoon S., advisor, Knowledge Institute of Medical Specialists (March 2016 – September 2016)
van Enst A., senior advisor, Knowledge Institute of Medical Specialists (from January 2017)
Belangenverklaringen
Conflicts of interest
The working group members have provided written statements about (financially supported) relations with commercial companies, organisations or institutions that are related to the subject matter of the guideline. Furthermore, inquiries have been made regarding personal financial interests, interests due to personal relationships, interests related to reputation management, interest related to externally financed research and interests related to knowledge valorisation. The statements on conflict of interest can be requested at the administrative office of the Knowledge Institute of Medical Specialists and are summarised below.
|
Member |
Function |
Other offices |
Personal financial interests |
Personal relationships |
Reputation management |
Externally financed research |
Knowledge-valorisation |
Other potential conflicts of interest |
Signed |
|
Workgroup |
|||||||||
|
Burger |
Advisor, Knowledge Institute of Medical Specialists |
None |
None |
None |
None |
None |
None |
None |
Yes |
|
Cobbaert |
Member, physician clinical chemistry |
Head of clinical chemistry department in Leiden LUMC. Tutor for post-academic training of clinical chemists, coordinator/host for the Leiden region Member of several working groups within the Dutch Society for Clinical Chemistry and member of several international working groups for clinical chemistry |
None |
None |
Member of several working groups within the Dutch Society for Clinical Chemistry and member of several international working groups for clinical chemistry |
None |
None |
None |
Yes |
|
Danse |
Member, cardiologist |
Board member committee of Quality, Dutch society for Cardiology (unpaid) Board member Conference committee DRES (unpaid) |
None |
None |
None |
None |
None |
None |
Yes |
|
Dekker |
Member, radiologist |
None |
None |
None |
None |
None |
None |
None |
Yes |
|
Geenen |
Member, radiologist |
Member Contrast Media Safety Committee of the European Society of Urogenital Radiology (unpaid, meetings are partially funded by CM industry))) |
None |
None |
None |
None |
None |
Has been a public speaker during symposia organised by GE Healthcare about contrast agents (most recently in June 2014) |
Yes |
|
Hoogeveen |
Member, nephrologist |
Member of Guideline Committee of Dutch Federation of Nephrology |
None |
None |
Member of Guideline Committee of Dutch Society for Nephrology |
Grant from the Dutch Kidney Foundation to study effect of fish oil on kidney function in post-MI patients |
None |
None |
Yes |
|
Kooiman |
Member, research physician |
Resident in department of gynaecology & obstetrics |
None |
None |
None |
None |
None |
None |
Yes |
|
Mostovaya |
Advisor, Knowledge Institute of Medical Specialists |
None |
None |
None |
None |
None |
None |
None |
Yes |
|
Oudemans – van Straaten |
Member, intensive care medical specialist Professor Intensive Care |
none |
None |
None |
None |
None |
None |
None |
Yes |
|
Pels Rijcken |
Member, interventional radiologist |
None |
None |
None |
None |
None |
None |
None |
Yes |
|
Sijpkens |
Member, nephrologist |
None |
None |
None |
None |
None |
None |
None |
Yes |
|
Vainas |
Member, vascular surgeon |
None |
None |
None |
None |
None |
None |
None |
Yes |
|
Van den Meiracker |
Member, internist vascular medicine |
None |
None |
None |
None |
None |
None |
None |
Yes |
|
Van der Molen |
Chairman, radiologist |
Member Contrast Media Safety Committee of the European Society of Urogenital Radiology (unpaid,CMSC meetings are partially funded by CM industry)) |
None |
None |
Secretary section of Abdominal Radiology; Radiological Society of the Netherlands (until spring of 2015) |
None |
None |
Receives Royalties for books: Contrast Media Safety, ESUR guidelines, 3rd ed. Springer, 2015 Received speaker fees for lectures on CM safety by GE Healthcare, Guerbet, Bayer Healthcare and Bracco Imaging (2015-2016) |
Yes |
|
Wikkeling |
Member, vascular surgeon |
None |
None |
None |
None |
None |
None |
None |
Yes |
|
Advisory Board |
|||||||||
|
Demir |
Member, physician clinical chemistry |
None |
None |
None |
None |
None |
None |
None |
Yes |
|
Hubbers |
Member, patient’s representative, Dutch Society of Kidney Patients |
None |
None |
None |
None |
None |
None |
None |
Yes |
|
Mazel |
Member, urologist |
None |
None |
None |
None |
None |
None |
None |
Yes |
|
Prantl |
Member, policy maker, Dutch Society of Kidney Patients |
None |
None |
None |
None |
None |
None |
None |
Yes |
|
Van den Wijngaard |
Member, resident clinical chemistry |
Reviewer for several journals (such as American Journal of Physiology) |
None |
None |
None |
None |
None |
None |
Yes |
Inbreng patiëntenperspectief
Patients’ perspective was represented, firstly by membership and involvement in the advisory board of a policy maker and a patients’ representative from the Dutch Kidney Patient Association. Furthermore, an online survey was organized by the Dutch Kidney Patient Association about the subject matter of the guideline. A summary of the results of this survey has been discussed during a working group meeting at the beginning of the guideline development process. Subjects that were deemed relevant by patients were included in the outline of the guideline. The concept guideline has also been submitted for feedback during the comment process to the Dutch Patient and Consumer Federation, who have reported their feedback through the Dutch Kidney Patient Association.
Methode ontwikkeling
Evidence based
Implementatie
In the different phases of guideline development, the implementation of the guideline and the practical enforceability of the guideline were taken into account. The factors that could facilitate or hinder the introduction of the guideline in clinical practice have been explicitly considered. The implementation plan can be found with the Related Products. Furthermore, quality indicators were developed to enhance the implementation of the guideline. The indicators can also be found with the Related Products.
Werkwijze
AGREE
This guideline has been developed conforming to the requirements of the report of Guidelines for Medical Specialists 2.0; the advisory committee of the Quality Counsel. This report is based on the AGREE II instrument (Appraisal of Guidelines for Research & Evaluation II) (www.agreetrust.org), a broadly accepted instrument in the international community and on the national quality standards for guidelines: “Guidelines for guidelines” (www.zorginstituutnederland.nl).
Identification of subject matter
During the initial phase of the guideline development, the chairman, working group and the advisor inventory the relevant subject matter for the guideline. Furthermore, an Invitational Conference was organized, where additional relevant subjects were suggested by the Dutch Kidney Patient Association, Dutch Society for Emergency Physicians, and Dutch Society for Urology. A report of this meeting can be found in Related Products.
Clinical questions and outcomes
During the initial phase of guideline development, the chairman, working group and advisor identified relevant subject matter for the guideline. Furthermore, input was acquired for the outline of the guideline during an Invitational Conference. The working group then formulated definitive clinical questions and defined relevant outcome measures (both beneficial land harmful effects). The working group rated the outcome measures as critical, important and not important. Furthermore, where applicable, the working group defined relevant clinical differences.
Strategy for search and selection of literature
For the separate clinical questions, specific search terms were formulated and published scientific articles were sought after in (several) electronic databases. Furthermore, studies were looked for by cross-referencing other included studies. The studies with potentially the highest quality of research were looked for first. The working group members selected literature in pairs (independently of each other) based on title and abstract. A second selection was performed based on full text. The databases search terms and selection criteria are described in the modules containing the clinical questions.
Quality assessment of individual studies
Individual studies were systematically assessed, based on methodological quality criteria that were determined prior to the search, so that risk of bias could be estimated. This is described in the “risk of bias” tables.
Summary of literature
The relevant research findings of all selected articles are shown in evidence tables. The most important findings in literature are described in literature summaries. When there were enough similarities between studies, the study data were pooled.
Grading the strength of scientific evidence
A) For intervention questions
The strength of the conclusions of the scientific publications was determined using the GRADE-method. GRADE stands for Grading Recommendations Assessment, Development and Evaluation (see http://www.gradeworkinggroup.org/) (Atkins, 2004).
GRADE defines four gradations for the quality of scientific evidence: high, moderate, low or very low. These gradations provide information about the amount of certainty about the literature conclusions. (http://www.guidelinedevelopment.org/handbook/).
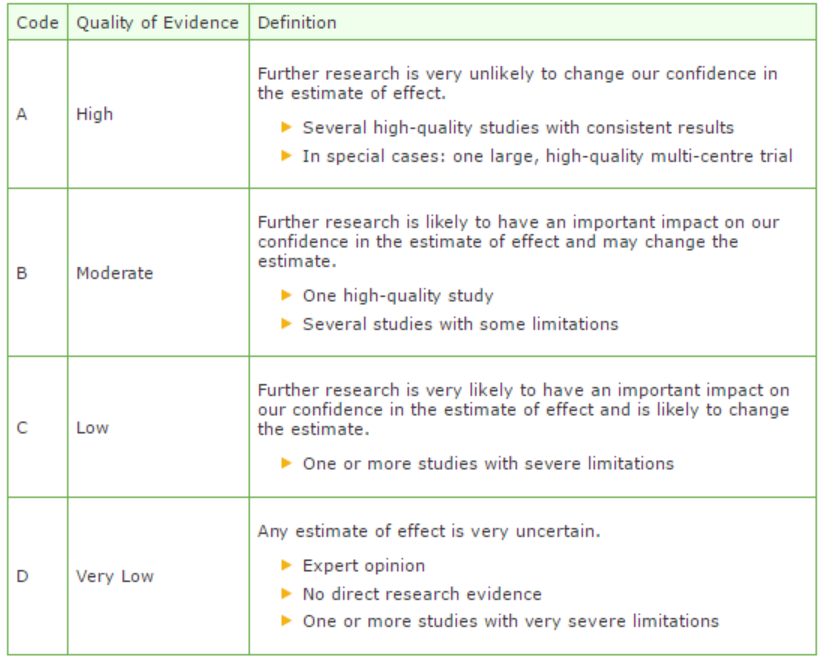
B) For diagnostic, etiological, prognostic or adverse effect questions, the GRADE-methodology cannot (yet) be applied. The quality of evidence of the conclusion is determined by the EBRO method (van Everdingen, 2004)
Formulating conclusion
For diagnostic, etiological, prognostic or adverse effect questions, the evidence was summarized in one or more conclusions, and the level of the most relevant evidence was reported. For intervention questions, the conclusion was drawn based on the body of evidence (not one or several articles). The working groups weighed the beneficial and harmful effects of the intervention.
Considerations
Aspects such as expertise of working group members, patient preferences, costs, availability of facilities, and organization of healthcare aspects are important to consider when formulating a recommendation. These aspects were discussed in the paragraph Considerations.
Formulating recommendations
The recommendations answer the clinical question and were based on the available scientific evidence and the most relevant considerations.
Constraints (organization of healthcare)
During the development of the outline of the guideline and the rest of the guideline development process, the organization of healthcare was explicitly taken into account. Constraints that were relevant for certain clinical questions were discussed in the Consideration paragraphs of those clinical questions. The comprehensive and additional aspects of the organization of healthcare were discussed in a separate chapter.
Development of quality indicators
Internal (meant for use by scientific society or its members) quality indicators are developed simultaneously with the guideline. Furthermore, existing indicators on this subject were critically appraised; and the working group produces an advice about such indicators. Additional information on the development of quality indicators is available by contacting the Knowledge Institute for Medical Specialists. (secretariaat@kennisinstituut.nl).
Knowledge Gaps
During the development of the guideline, a systematic literature search was performed the results of which help to answer the clinical questions. For each clinical question the working group determined if additional scientific research on this subject was desirable. An overview of recommendations for further research is available in the appendix Knowledge Gaps.
Comment- and authorisation phase
The concept guideline was subjected to commentaries by the involved scientific societies. The commentaries were collected and discussed with the working group. The feedback was used to improve the guideline; afterwards the working group made the guideline definitive. The final version of the guideline was offered for authorization to the involved scientific societies, and was authorized.
References
Atkins D, Eccles M, Flottorp S, et al. GRADE Working Group. Systems for grading the quality of evidence and the strength of recommendations I: critical appraisal of existing approaches The GRADE Working Group. BMC Health Serv Res. 2004 Dec 22;4(1):38.
Van Everdingen JJE, Burgers JS, Assendelft WJJ, et al. Evidence-based richtlijnontwikkeling. Bohn Stafleu van Loghum. Houten, 2004
Zoekverantwoording
Zoekacties zijn opvraagbaar. Neem hiervoor contact op met de Richtlijnendatabase.